{kind=link}
Here's something you might be interested in.
Ask a Hipster — Advice you didn't know you needed
Big Screen — Movie commentary
Blurt — Music's inside track
Booze News — San Diego spirits
Classical Music — Immortal beauty
Classifieds — Free and easy
Close to Home — What it’s like on the street where you live
Cover Stories — Front-page features
Drinks All Around — Bartenders' drink recipes
Excerpts — Literary and spiritual excerpts
Feast! — Food & drink reviews
Feature Stories — Local news & stories
Fishing Report — What’s getting hooked from ship and shore
From the Archives — Spotlight on the past
Golden Dreams — Talk of the town
The Gonzo Report — Making the musical scene, or at least reporting from it
Letters — Our inbox
Movies@Home — Local movie buffs share favorites
Movie Reviews — Our critics' picks and pans
Musician Interviews — Up close with local artists
Neighborhood News from Stringers — Hyperlocal news
News Ticker — News & politics
Obermeyer — San Diego politics illustrated
Outdoors — Weekly changes in flora and fauna
Overheard in San Diego — Eavesdropping illustrated
Poetry — The old and the new
Reader Travel — Travel section built by travelers
Reading — The hunt for intellectuals
Roam-O-Rama — SoCal's best hiking/biking trails
San Diego Beer — Inside San Diego suds
SD on the QT — Almost factual news
Sheep and Goats — Places of worship
Special Issues — The best of
Street Style — San Diego streets have style
Surf Diego — Real stories from those braving the waves
Theater — On stage in San Diego this week
Tin Fork — Silver spoon alternative
Under the Radar — Matt Potter's undercover work
Unforgettable — Long-ago San Diego
Unreal Estate — San Diego's priciest pads
Your Week — Daily event picks
A visit to a Tijuana morgue
Baja anatomy professor: My students learn compassion.
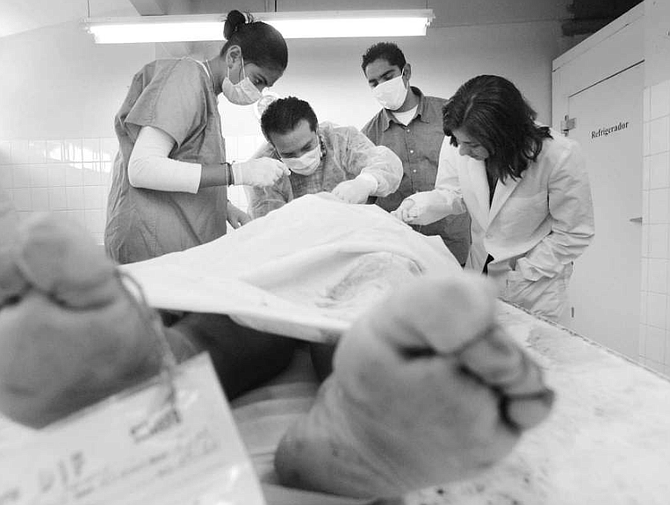
Dr. Luis Antonio Martínez and student. “Every week, while I’m driving to the university to do a dissection, I apologize to the people whose bodies we use."
"Doctors, dentists, surgeons don’t have to guess about what they’re doing. Where to cut. How to cut. How to suture. All that knowledge comes from human dissection, from studying the bodies of the dead."
Not long after my brother died and was buried in Oregon, I found myself in the depósito de cadáveres, or morgue, at Tijuana’s Autonomous University of Baja California. My hand rested on the handle of a large walk-in refrigerator. I wasn’t sure what I’d see inside.
Earlier in the day I attended a one-hour lecture given by Dr. Luis Antonio Martínez, a dental surgeon who teaches anatomy to students at the university’s dentistry school. His lecture was attended by 20 first-year students, of whom only 2 were male. Dr. Martínez was preparing his students for their first cadaver dissection. On the blackboard he drew a simple human face — ears, eyes, nose, mouth, chin.
“Next week you will first make a straight, horizontal, seven-centimeter incision two centimeters below the lip.”
The students, all in their early 20s, copied Dr. Martínez’s drawing of a face and his instructions into their notebooks. Dr. Martínez described how the students were to make three shallow incisions into the cadaver’s chin.
“Then you will take the top left corner of this trapezoid in your clamps and, inserting your scalpel at a 45-degree angle into the incision, begin carefully to cut, separating the skin from the tissue beneath.
“As you cut and pull away the skin, you will first see fat, which is yellow. You may also see muscle tissue, which, depending on the freshness of the cadaver, will be either deep pink or light brown.”
The young woman sitting next to me shuddered but didn’t look up. She wrote in her notebook “muscle tissue, deep pink, light brown.” Her fingernails were painted glittery red.
Dr. Martínez went on to describe three muscles his students would reveal beneath the skin and fat.
“And at the end of the dissection, I will show you why dissection is important. I will show you the precise points you will need to inject in order to anesthetize either the right or left front corner of the mouth. You’re going to see exactly where these points are, between the first and second bicuspid. When you work with patients, you won’t be able to see these points beneath the tissue. You will have to visualize them in your mind. By dissection, you will have a clear picture of where they are.”
Dr. Martínez, in khakis and pressed white shirt, his complexion fair, his skin unwrinkled, his thick dark hair combed straight back, didn’t look much older than the students he lectured. He is a 33-year-old father of three who, in addition to lecturing at the university two days each week, owns and runs two dental clinics. On a busy day like a Saturday, each of his clinics may see as many as 20 patients.
“I don’t have to teach,” Dr. Martínez told me. “But I love to teach. I like being around young people, their energy. When you’re my students’ age, you have everything to look forward to. You have all these dreams for your future. You get older, things change. Not long ago I was thinking about this, and I realized, ‘Hey, that future I used to dream about when I was young — I’m living that future now!’ ”
Dr. Martínez has been teaching anatomy at the university since he was 26 years old.
“You may notice that there are very few boys in my class. In Mexico, boys want to be doctors, not dentists. Boys have this idea that dentistry is delicate work, feminine work. It’s an entirely wrong idea. But I was like that. When I first went to university, I wanted to be a doctor. I had almost completed my first year of medical school when my grandmother was diagnosed with uterine cancer. My father wanted to do whatever was necessary to help her. He told me, ‘Son, the next year or so is going to be financially difficult for our family. I’m afraid you’re going to have to quit school for a while and get a job.’
“I went to San Diego and got a job as a waiter at Anthony’s. I loved it. On a good night, I could make $100 in tips. And they had jazz. That’s where I learned to love jazz. But my poor grandmother. The family spent over $120,000 on getting her the best medical care, on making sure she stayed in the best hospitals. But in the end, no matter how hard we tried, nothing could save her.
“When I went back to school, it was too late to enroll in the medical school’s second-year program. I would have had to wait another year. Professors on the dentistry school faculty said, ‘Come on! Study with us! You can start right away.’ I enrolled in the dentistry school, and I loved it immediately. I especially loved being able to continue the study of human anatomy.
“Even when I was a child, I was fascinated with the human body. I remember I saw the movie Frankenstein, and it was just amazing. The idea of a human body having different working parts, like a machine. I wondered how the body worked. I wanted to know how it was put together.
“From the very first time I participated in dissecting a cadaver, in the year I spent in medical school, I was overwhelmed by what a tremendous privilege it was to be able to examine the human body and learn in a very precise, detailed way how it worked. It’s really an honor to have that opportunity.
“When I finished dentistry school, I had done so well in anatomy that my professors asked me to take an additional two-year course of study in the subject so I’d be able to teach it. They felt that students of general dentistry, and not just dental surgeons, should have the opportunity to do dissection. So, anatomy is all I did for two years. Anatomy and dissection. And then I started to teach, which was a little strange because I was only a few years older than many of my students. I had to work hard to gain their respect. I had to show them, in a careful, thoughtful way, that I knew what I was talking about, that I was competent.”
On the afternoon Dr. Martínez and I met to talk, after he’d given his lecture on chin dissection, we sipped icy Cokes outside the university’s food court. Inside, students lined up before franchises for pizza, hamburgers, Chinese food, Mexican food, health food. Dr. Martínez explained to me that general dentistry students at the university paid around $160 in tuition per semester and that a degree in general dentistry usually took five years, or ten semesters, to complete. After the students graduate, the government requires that they spend one year practicing at a government-run clinic. He went on to tell me that in their first semester, the students study general anatomy, and in their second semester, descriptive anatomy of the head and neck, and then topographic anatomy of the head and neck by dissection. Dr. Martínez invited me to attend on the following Tuesday his class’s first cadaver dissection. A hot, dry wind was blowing from the northeast across the campus. My eyes watered and my mouth was dry. I asked if I might first see the morgue.
“Of course,” he said. “I understand. It’s best to approach these things little by little.”
He led me across campus to a low-slung, recently built structure with many windows set high in its beige walls. He led me into the immaculate white-tiled dissection room. He showed me the six waist-high, white-tiled dissection tables, each equipped with a water hose and a shiny stainless steel drain. In the northwest corner of the room, the walk-in refrigerator hummed.
“I don’t know how many we have today,” Dr. Martínez said, gesturing to the refrigerator. “If you want to look inside, you may.”
The day after my brother died, I went to the small Oregon town where he’d lived. I saw his body at the mortuary. He’d just been delivered from the coroner. I knew in my mind that he was dead. The mortician opened the door to the room where my brother lay. I saw my brother’s body. My knees gave out from under me.
At the university’s morgue, with Dr. Martínez watching, I opened the walk-in refrigerator. Cold air poured out. The refrigerator’s interior was dark. My eyes took several seconds to adjust. I saw three bodies lying on white gurneys. Blood-spattered muslin sheets covered the bodies. The air smelled of old blood.
Dr. Martínez asked, “So, do you think you’ll be able to attend our first dissection?”
“I think I’ll be fine,” I said.
“I apologize to them.” Dr. Martínez took me by the elbow. “Every week, while I’m driving to the university to do a dissection, I apologize to the people whose bodies we use. It’s not really a prayer. It’s just something I say in my mind. An apology for what we do.”
Greek religion prohibited the desecration of corpses. But it was the Greeks who were the first to take a scientific interest in human anatomy. By the Sixth Century BCE, the Greek treatment of disease had moved away from magic and spells, and the philosopher Alcmaeon conducted the first recorded attempts at human dissection, allowing him to discover, for example, the difference between arteries and veins. Later, Plato and Aristotle taught that body and soul were separate. This notion that the body was only a shell meant that cutting on a cadaver mattered little and helped assuage the public’s disgust at the practice. By 237 BCE Herophilus of Chalcedon, a follower of Hippocrates, established the world’s first school of anatomy in Alexandria, Egypt. But people remained uncomfortable with human dissection. The advent of Christianity and the doctrine of bodily resurrection gave further reason to the public’s discomfort. Whether the Catholic Church ever officially prohibited human dissection is unclear. Some medical histories contend that the Church banned the practice. The National Catholic Bioethics Center in Boston and the Catholic Encyclopedia assert that the Church never banned the practice, and they cite numerous instances of medieval scientists in Catholic countries who conducted human dissection without Church interference.
Two centuries after Martin Luther’s death, physicians throughout Western Europe knew that without dissecting cadavers, the systematic study of human anatomy was impossible. So began what some medical historians have called the “great cadaver shortage.”
The 18th Century witnessed scenes of people scrambling to steal corpses and sell them to physicians. The bodies of the anonymous poor were always up for grabs. In London, people fought over the bodies of executed criminals. The demand for cadavers was so great that some physicians resorted to grave robbing. Public sympathy for this trend was also in short supply. In 1788, 5000 New Yorkers rioted for three days after they learned that medical students at the Hospital of the City of New York were dissecting bodies stolen from a local graveyard. And today there are professors of literature who believe that this anger, fear, and suspicion were so pervasive that they played in Mary Shelley’s imagination when in 1818 she wrote Frankenstein.
A hot, dry wind was blowing on the early afternoon Dr. Martínez and his students met at the university morgue for the first dissection. We gathered in an anteroom where we put on gauzy blue surgical gowns, surgical masks, latex gloves, and blue surgical booties. A few of the girls giggled. Dr. Martínez joked with the students about how they looked in their surgical garb, about how they struggled to get the tight gloves over their sweaty fingers.
“I try to keep it light,” he later told me. “The first time is difficult.”
We pushed through the swinging doors into the dissection room. Dr. Martínez stood before us and clapped his gloved hands together.
“This isn’t a surgical setting, but I want you to behave as though it were. Once your hands touch anything in this room, your gloves are no longer sterile. Be careful not to rub your eyes or touch your mouths. Be conscious of where your hands are and what they’re doing.”
He asked two students to enter the walk-in refrigerator and wheel out the cadaver on the far left. Four young women darted to a bench on the dissection room’s far side, where they sat with their hands wedged under their thighs. Dr. Martínez pretended not to notice.
“You can’t play into the students’ fears,” he later told me. “You can’t create a fearful situation. I know a story of one professor who taught at another university, who was a very religious man and who was very nervous about doing human dissection. He would sweat. He would shake. He communicated his discomfort to his students. Some of them fainted. After one dissection, while he was closing an incision, he pricked his finger with the needle. A month or so later, he developed a small tumor in his finger right where he had pricked himself. He had the tumor removed. A few months later, the tumor reappeared. Again the tumor was removed. When the tumor was analyzed, it was determined that the tumor was somatic in origin. In other words, the professor was so nervous about doing human dissection, he was so worried about it, that his body had actually produced these tumors in his finger.”
When the students wheeled the cadaver into the dissection room, everyone grew quiet. Dr. Martínez and I each gripped two corners of the sheet in which the cadaver was wrapped and, grunting, lifted the body from gurney onto dissection table. Dr. Martínez pulled back the sheet to reveal the cadaver’s face: a dark-skinned young man with a head of thick, long black hair. His congealed eyes were half-open, his pupils were dime-size. He had stubble on his cheeks and chin, and, beside his left nostril, a small crusty purplish hole.
Dr. Martínez bent to examine the wound. “He was probably shot with a .38.”
“He looks so peaceful,” one of the students said.
“He probably didn’t die immediately,” Dr. Martínez said. “From his relaxed expression, I’m guessing it took him several minutes.”
One of the students, a young man, volunteered to play the role of surgeon. He took a black marking pen and drew the required trapezoid on the cadaver’s chin. Taking his scalpel, he started to cut, following the outline. Two girls seated on the bench wandered over to watch. One reached out to touch the cadaver’s shoulder.
“He’s cold,” she said. “And hard.”
When the three incisions were completed, the young surgeon folded back the skin.
“The yellow tissue is fat,” Dr. Martínez said. “I want you to remove it so you can see the three muscles I told you about.”
And the young surgeon, with tweezers and scalpel, started removing the yellowish pea-size globules. With delicacy he placed them on a pink surgical napkin that another student had draped across the cadaver’s naked brown chest. When the three muscles were revealed, Dr. Martínez asked the young surgeon to scrape them from the jawbone. “I want to show you the small hole in the jaw from which the nerve I told you about emerges.”
I could hear the sound of blade scraping bone. I examined the dead man’s feet.
“Notice his toenails,” Dr. Martínez told me. “They’re infected with fungus. We see that often in the cadavers we get. Many are migrants to Tijuana from rural southern Mexico, where people wear sandals and their feet have a lot of contact with soil. You can also tell he wore sandals from the calluses on the soles of his feet.”
The cadaver’s toe tag said he was an unidentified male, 25 to 30 years old, and that he’d been found on February 19, 2002, in Sanchez Díaz, a Tijuana neighborhood Dr. Martínez described as “violent.”
“Many bodies are found there. Drugs. Drug dealing. These people come up from the south to find work in Tijuana or cross into America, and they get mixed up in drugs.
“Fifteen years ago in Tijuana, we didn’t have enough cadavers for our medical students. Sometimes UCSD would send us some. Now everything has changed. The drug cartels. Thousands of migrants from the south. Tijuana has become so violent, we have plenty of cadavers. This is something very new in our city’s history.”
Sixteenth-century Spaniards brought the practice of human dissection to Mexico. Dr. Frank Gonzalez-Crussi, former head of pathology at the Children’s Memorial Hospital in Chicago and professor emeritus at Northwestern University, explained to me how this happened.
“The exact date is unclear. I’m guessing it was in the late 1500s, after the Conquest was completed. There was an outbreak of bubonic plague in Mexico City, and Spanish physicians, who’d arrived with the Conquistadors, dissected several plague victims at the Hospital de Jesús in Mexico City. That is the first known instance of scientific dissection in Mexico.
“What is remarkable about this is that we know that the Aztecs for centuries practiced human sacrifice. There’s some debate about the actual numbers of human sacrifices — hundreds, thousands, ten of thousands. We do know that they sacrificed at least hundreds of people. The Aztec priests would cut open the victim’s chest and offer his heart to the god Huitzilopochtli. What is interesting is that these priests, who had no qualms about cutting open a human body, showed no interest in the body’s organs, how the body was put together, how it worked. Despite all the many great achievements of Aztec civilization, in architecture and astronomy, the Aztecs took no interest in human anatomy. There’s no historical evidence that they ever made any attempt at all to study human anatomy.
“They didn’t see the human body in the same way as the Spaniards did. And this is a very important point to understand. Cultures literally see things in different ways. When the Aztecs opened a body, they didn’t see it as a kind of machine that had different working parts. For them, the body had a mystical significance.”
What is remarkable about Gonzalez-Crussi is that he is an immigrant from a poor Mexico City family who became, according to those who’ve reviewed his books, “America’s most beautifully eloquent writer on the subjects of pathology and human anatomy.” He’s authored seven books. He writes articles for the New Yorker. His most recent work, There Is a World Elsewhere, a memoir published in 1998, received excellent reviews in the Washington Post, the New York Times Book Review, and the Chicago Tribune. In 2001 he was named a Guggenheim Fellow and used the grant to complete his eighth book, “a book about birth. I began with a book about death and have written often about death, and now I’ve come full circle.
“Even as a child I knew I wanted to write, but I grew up in a proletarian neighborhood where wanting to be a writer could be only a kind of dream. I describe where I grew up in There Is a World Elsewhere. By the time I finished medical school in Mexico City and came to the States to complete my studies, I was absorbed in my career. Medicine is all-consuming. It requires not only enormous energy, but to move further, to make your way in the discipline, not to mention becoming a professor, takes up most of your life. When I was in my 50s, I decided it was time to write. I decided, ‘It’s now or never.’
“And I wrote about what I knew. Pathology. Human anatomy. Death. And I perhaps thought I could write about these things in a literary way because I grew up in Mexico, and there is a difference between the ways Mexicans and Americans regard death. I grew up with the Day of the Dead — I even ultimately wrote a book about it. Although my family didn’t make a shrine, or ofrenda, for the Day of the Dead, our neighbors certainly did. And there was this sense in Mexico that the dead are present with us. We don’t absent them. We want to keep in conversation with them. The familiarity with death is a little more in the air in Mexico than it is here in the United States.
“When I first arrived in America I was clearly told that death was something one didn’t discuss in ‘polite society.’ One colleague told me that discussing death or pathology in a social setting was like discussing pornography. It simply wasn’t done. Things have, of course, changed somewhat, but when I first got here, discussing death anywhere outside a clinical setting was taboo.
“Of course, the great irony of this was that the United States had become preeminent in the world not only for the study of pathology and human anatomy, but for medical science in general. This was a huge change. Before World War II, Germany had been the world’s great center for the systematic study of human anatomy. Even into the late 19th Century, the systematic study of human anatomy hadn’t truly evolved as a discipline at the University of Mexico City. Mexican doctors who wanted to study pathology and human dissection went to Germany, or to Austria, which was also very strong in those fields.
“There are some people who may disagree with me, but the systematic study of human anatomy didn’t truly become a discipline in Mexico until the 1920s, when President Lázaro Cárdenas accepted many Spanish refugees who were fleeing Franco. In many instances, these people were la crème de la crème of the Spanish intelligentsia. One of these refugees, Isaac Costero, who’d studied in Germany, really founded anatomical pathology as a discipline at the University of Mexico City.”
I asked Dr. Gonzalez-Crussi if, after his many years as a pathologist, he’d ever grown used to human dissection.
“No. Not even after many years. You do develop some tolerance, but no, it never becomes just a job. I suppose there are some callous people for whom the practice might become routine. In some ways the spectacle of autopsy is such that it may lead some people to think of the body only as a machine. Most doctors are inspired by that kind of philosophy. They may tell you that the human body is a wonderful machine, but it’s still a machine. The workings of a machine may be more or less completely understood.
“That we are animal, that we are mechanical, I have no doubt. But it can’t be reduced to that and nothing else. We may completely understand the anatomy of the human brain, but we can’t explain what composes a symphony in the brain of a composer. Thoughts cannot be explained only by mechanism.
“And this is part of the mystery revealed by the spectacle of the cadaver. This is why human dissection is so impressive. It underscores all these questions. And, most significantly, when confronted with a cadaver, you can’t deny the reality of all it implies. The cadaver points to the path which all of us without exception will follow.”
I asked Dr. Gonzalez-Crussi whether he’d ever gotten used to his work because two weeks after the first dissection, I returned again to Tijuana to attend another. Dr. Martínez had explained to me that the purpose of the first dissection was to acquaint his students with the process itself.
“I want them to get over their fears, their nervousness, so they can actually start seeing the body in an objective, scientific way. I don’t want them ever to learn to disrespect the cadaver or treat it casually. I’ve suspended students even for making unnecessary incisions on cadavers. But I want them to see the human body objectively. In order to work on living people, you have to. That’s why physicians and dentists almost never treat family members. It’s almost impossible to look objectively at the body of someone you love. When you’re dealing with someone you love, it immediately becomes subjective. I’ve tried a couple of times to work on my children’s teeth, but it was impossible. If I hurt them, for example, when I gave them an injection, and they started to cry, it was unbearable for me. I’d hurt my child. They’d start crying, and I’d almost feel like crying myself.”
The second cadaver was that of a strong, handsome, broad-shouldered young man. His toe tag said he was unidentified, between 19 and 22 years of age, and that, on February 2, 2002, he’d been hit by a car while crossing the old road to Tecate. He was so heavy that we couldn’t lift him from his gurney.
Dr. Martínez pulled back the sheet. The young man’s right side, from armpit to hip, was covered with dark bruises and deep lacerations. His right shin, just below the knee, had been fractured completely. Broken bone poked through skin, revealing sinew and muscle. Below the fracture, the leg could be moved back and forth, as if it swung on a hinge. The young man’s brown belly was distended. Dr. Martínez explained that he’d suffered massive internal injuries. And that was why, Dr. Martínez said, the cadaver had a high smell.
The odor was cloying. I could smell it even through my surgical mask — a very strong meaty odor. Unpleasant. Something that couldn’t be gotten used to. Hours after I left the dissection, had driven home from Tijuana, showered, brushed my teeth, changed clothes, settled in for the night, the smell stayed with me. (A doctor friend later told me, “The trick is to smear a little Vicks VapoRub on your upper lip or on the inside of your surgical mask. It helps.” Dr. Martínez later told me, “I always drink a lot of coffee before a dissection, so when I’m breathing in my surgical mask, the only thing I smell is coffee.”)
Perhaps it was because of and not despite this odor, and the sheer size of the cadaver, that the reality of the human body as flesh was clearer to me. Witnessing the second dissection was easier. Dr. Martínez’s students, too, were more at ease. No one ran off to sit on a bench. Everyone gathered around the gurney. A young woman volunteered to play the role of surgeon. She began to make the same trapezoid-shaped incision on the cadaver’s chin.
“This time,” Dr. Martínez said, “we’re going to proceed more carefully, more slowly, as if we were operating on a living patient.”
The young woman was very precise. She took her time. While she worked I asked Dr. Martínez if he ever wondered about the lives of the people his students dissected.
“It’s inevitable. They’re human beings. And you wonder what their story was, what brought them to the dissection table. Every now and then we get a young man with the words ‘Mara Salvatrucha’ tattooed across his chest or back. From watching the news, I learned that this was the name of a Salvadoran gang that preys on people crossing the Mexican-Guatemalan border. But why do they end up dead here, in Tijuana? Over the years, I’ve seen certain patterns emerge. We get more suicides during the winter when people become depressed and drink more. We get more women during the summer months, when there are more parties, when men go out drinking and looking for women. We get a lot of prostitutes. Women from the interior of Mexico who come north looking for work, and the only work they can find is prostitution. Some of them end up dead. Found strangled or smothered in a hotel room. I remember one woman in particular. She had been strangled. She had stretch marks that suggested recent pregnancy. And her breasts where swollen, as if she’d been nursing. She had, I noticed, track marks on her arms. She’d been using drugs. And I couldn’t stop thinking about her. A child, somewhere, had lost his mother.”
When the young woman had completed her dissection of the cadaver’s chin, had peeled back the skin, removed the fat and muscle, Dr. Martínez took charge. He pointed to a small hole in the cadaver’s chin from which emerged a thin, pearly-white strand of tissue.
With a pair of tweezers Dr. Martínez pulled at the strand, what Gray’s Anatomy identifies as the mental nerve. (“Mental” in this case coming from the Latin mentum, relating to chin, and not from mens, relating to the mind.)
“This is the nerve I told you about. And it’s exactly right where I told you it would be, directly below the first and second bicuspid.”
Dr. Martínez pulled back the cadaver’s lip and inserted a probe between the gum and lip, beneath the first and second bicuspid. He poked the probe through the tissue, and it emerged precisely at the mental nerve’s base.
“You see, this is where you must insert your needle when you need to anaesthetize this part of the mouth. Now that you’ve seen where the nerve is located, you can have a clear picture in your mind when you’re working on a patient. This is why dissection is so important.”
In Mexico, it can also be lethal. There are Mexicans who, for reasons other than religious or moral, prefer that the dead remain untouched. In Mexico, forensic pathology can be dangerous.
In an idle moment, Dr. Martínez told me about Dr. Irma Rodríguez, who, until July 2001, worked as medical examiner for Ciudad Juárez, just across the border from El Paso.
“There aren’t a lot of people in Mexico who want to study forensic medicine or dentistry. At the university here, they only offer a six-month course in those subjects every now and then. I took a course in forensic dentistry because it interested me. I do it only as a sort of a hobby. Maybe two or three times a year, a family needs a body to be identified and they’ll have dental records. It’s actually not very complicated to do.
“But Dr. Irma Rodríguez was involved in identifying bodies found in mass graves that had been discovered in ranches outside Ciudad Juárez. Everyone knew that the drug cartels were involved. Everyone knew that these mass graves existed. Everyone knew that the authorities were aware of the mass graves. And everyone knew that the drug cartels didn’t want the bodies found in those mass graves to be identified. Dr. Rodríguez must be a very brave woman. As I said, few people in Mexico study forensic medicine.
“What happened in July of last year was that someone, it isn’t clear who, shot and killed Dr. Rodríguez’s husband and daughter. From what I understand, Dr. Rodríguez was away at the time, attending a conference in Mexico City. Dr. Rodríguez’s daughter was driving Dr. Rodríguez’s car. And there are some people who believe that the gunmen mistook the daughter for Dr. Rodríguez. The details aren’t clear. Someone wanted to send a message. Someone didn’t want the bodies in those mass graves to be identified. Someone wanted to send a message that Mexico wasn’t perhaps the best place to make a career in forensic dentistry or medicine, at least not in Ciudad Juárez.”
I was in the lobby of the Tijuana medical examiner’s office, Servicio Médico Forense de Tijuana, on the morning of April 11 — the morning after Tijuana’s chief of police, Carlos Otal, and 200 other law enforcement officers, were arrested by Mexican federal authorities. I was studying a sign posted in the lobby that said, We Respect Your Pain: We Accept Neither Gifts Nor Gratuities for Our Services, when several plainclothes officers walked in. They wore tailored shirts and snug Calvin Klein jeans and freshly polished boots. They had tucked guns under their waistbands. They were gossiping about the previous day’s scandal. It sounded as though Chief Carlos Otal, at the time of his arrest, reacted with less dignity than was expected from a public official confronted with a touchy situation.
“He screamed, ‘You’re treating me like a common criminal!’ ” one of the plainclothesmen said.
“He yelled, ‘Hey, be careful! You’re getting my pants dirty!’ when they were dragging him away.”
I was at Servicio Médico Forense de Tijuana on Boulevard Fundadores, just a block or so south of Happy Chicken restaurant, because I wanted to speak with the servicio’s director, Dr. Luz Vertila Ontiveros. But la doctora was late. I went outside the lobby for a cigarette. While I smoked, the wind blew a sheet of old newspaper at my feet, a page from the February 27, 2002, edition of El Mexicano.
An article entitled “One Shot to the Head” described the execution-style slaying of a 36-year-old man who lived in a Tijuana neighborhood called the Hills of Friendship. Another article described the arrests of four kidnappers who, in a residence near the intersection of Kiwi and Strawberry Streets, had held captive a woman named Nancy. Another article detailed how a group of six young men armed with high-power weapons had “with extreme violence” kidnapped a 40-year-old man. The group’s leader, the article said, “was presumed to have dedicated his life to the sale of drugs.”
Dr. Luz Vertila Ontiveros, a pretty and coquettish woman in a pristine lab coat, told me she oversees between 800 to 1000 autopsies each year.
“I can’t give you a more precise figure because it varies. I’ve been here for seven years, and each year the numbers have been different. What I can tell you is that we have a staff of nine forensic examiners and we receive the bodies of people who die unattended, outside a hospital or doctor’s care. We also receive the bodies of people who die in hospitals but who have no family. And we, of course, get the bodies of people who die of unnatural causes. Crime victims. Bodies that have been left somewhere.
“I’d estimate that between 10 and 20 percent of the bodies we receive are unidentified. We take their dental impressions, their fingerprints. We take pictures of them. By law we’re required to hold unidentified bodies for ten days. After that, we hand over our autopsy reports and identification materials to the state judicial office. Of those unidentified bodies, we send several every week to the university for dissection by medical and dentistry students. The bodies must be intact and in good condition. We clean and embalm them. We also test them for HIV. Only HIV-negative cadavers are sent to the university. The rest of the bodies are sent to a municipal cemetery and are buried in a common grave, as are the cadavers used at the university after the students are done studying them.”
I asked the doctor if she’d heard of Irma Rodríguez. She paused.
“Well, of course. Forensic medicine is a dangerous profession in Mexico. But, here, we’re left alone. We work for the city. We do our job. No one bothers us.”
Panteón Numero 11, Municipal Cemetery Number 11, is where Tijuana for the past two years has sent its unidentified dead for burial. (The ten other municipal cemeteries can no longer make room for them.) To get to Municipal Cemetery Number 11, you take the Via Rápida, or freeway, that runs from Zona Rio to the far southeast of Tijuana. The Via Rápida’s on-ramps are difficult to navigate and offer even the most skillful driver an intimation of mortality. On the afternoon I managed to get onto the Via Rápida, an old white pickup rumbled in front of me for many miles. In the back of the truck bounced four rusty drums. Written in big red block letters on the tailgate were the words Material Peligroso, Dangerous Material.
Municipal Cemetery Number 11 sits a mile or so behind Mount of Olives, a well-kept and privately owned cemetery for the city’s middle and upper classes. To get to Municipal Cemetery Number 11 you turn right at the Mount of Olives’ entrance and continue up a rocky and deeply rutted road.
“We serve the people” is what one of the municipal cemetery’s workers told me as he led me to where the unidentified are buried. “It costs maybe $50 for a family to bury someone here. It’s inexpensive and their family member can have a dignified grave.”
The unidentified rest at the bottom of a steep hill. A thin metal spike marks each common grave, each grave holding, I was told, 10 to 20 bodies. In this southeastern part of Tijuana, the hills are brown and barren. Across from the common graves, a hundred or so yards away, stand several ramshackle homes built by squatters. When the wind was right I could hear domestic noise from those homes — a woman calling for her children, a rooster crowing. Wild mustard glazes a gully that runs beside the common graves. Plastic Coke bottles, transistor batteries, an old hairbrush litter the earth covering the common graves.
Up the hill, people have surrounded many of the $50 graves with small white picket fences. Other families have provided not only small white picket fences but have also hauled patches of fresh sod to Municipal Cemetery Number 11 and planted them atop the graves. The headstones on these more elaborate $50 graves look like small houses, and they hold pictures of the deceased. From their perspective, the deceased stare out at a patch of green lawn surrounded by a white picket fence, the sort of view afforded by the living-room window of a suburban dream home.
Plastic flowers and bits of ribbon sometimes drift down to the common graves. If anyone has ever visited them, they’ve left no sign. I counted 118 thin metal spikes. There were probably more, but the air at the bottom of the hill was hot and oppressive, and small black flies worried my forearms and back of my neck. I made my way back up the hill. Two funerals were in progress. I could see another hearse making its way up the long, rocky, rutted road. A Popsicle salesman trundled his cart toward one of the funerals. Not far from the other funeral sat a little boy on an upturned blue bucket. He was selling plastic sacks of pork rinds to the mourners.
Dr. Martínez’s main office sits on Third Street in downtown Tijuana, between Constitución and Niños Héroes, at the entrance to a large yellow parking garage. I went to visit him at his office not long after I’d visited Municipal Cemetery Number 11. The news on my car radio that morning concerned troubles at the Los Angeles medical examiner’s office.
“I know there have been reports of rats gnawing at the bodies in our care,” an L.A. forensic examiner said. “But we’re really not talking about gnawing here. We’re talking about a full-on meal.”
I found Dr. Martínez in good spirits. He’d just learned that a team of Cuban physicians was coming to the university to offer a certificate program in oral pathology.
“I’m going to take the course,” he told me. “The only thing is that you have to take the final exam in Havana. But, you know, that’s sort of my dream. To keep on learning. I think that if I work hard enough, someday, after my children are raised, that’s all I’ll do. I’ll take courses and maybe write a little.
“For the past two years I’ve been writing a textbook for dentistry students on head-and-neck dissection. Right now, they have to buy a general text on dissection that costs around $50. My book would cost only $6 or $7. And it’s written specifically for general dentistry students.
“I think it’s this kind of attention that makes our students the best in Mexico. Every year, there are seminars for dentistry students, and they take national exams. Every year our students have the highest scores. The quality of education here is very high. We have a close relationship with the dentistry school at UCSD. From them we learn about all the newest advances in American dentistry. They help us acquire the latest equipment. Our quality of care here is very high. I say this knowing that there are dentists in San Diego, in America, who tell people not to come to Tijuana for dental work. They say that we’re dirty. That we don’t sterilize our equipment. It’s sort of ridiculous. I have friends who work at certain dental clinics in San Diego, clinics that deal mostly with immigrants. My friends work as dental assistants. I hear horror stories.”
Dr. Martínez offered to take me for an early lunch at a fish taco restaurant near Guerrero Park. I accepted and when we arrived Dr. Martínez immediately ordered for himself tacos made of manta ray.
“I compartmentalize very well,” he said, shaking hot sauce onto his tacos. “I don’t let associations from one thing carry over to another. At home, I don’t talk about dentistry or dead people. At the clinic, I don’t talk about my personal life. I keep things separate. Right now, I can talk about my work at the university, and it wouldn’t bother me.”
I asked him if, after all these years, his work in dissection didn’t at times bother him.
“Several instances come to mind. I remember a couple, a boy and a girl, maybe 15 or 16 years old. This was maybe three years ago. They’d both been shot in the back of the head with a shotgun. From what I understand, when their bodies were found, they were still holding hands. They were in some gully. In some ravine. They’d been shot in the back of the head. Why?
“Two years ago, there was an eight-year-old boy. You know, one of the kids who just lives on the street. And he’d been stabbed. He died of multiple stab wounds to his abdomen. He was just one of those kids that we now have in Tijuana that just lives in the streets. No one claimed him. He was unidentified. I have children of my own. And there was this little boy. I sort of cuddled his body. I spoke to him gently because, I thought, maybe no one in his life had ever cuddled him or spoken to him gently.
“And of course I didn’t use him for dissection. I can’t. I understand that for the medical school it’s very important that they learn pediatric anatomy. That’s how they learn to care for children. A child’s anatomy is so different from that of an adult. But I’ve never been able to use a child for dissection. A year or so ago there was an 11-year-old girl. She was raped and strangled. You could still see the finger marks on her throat. And so, no. No. To cut her face? No.
“And not long ago they sent us a cadaver with no face. It was a young male. Maybe 20 years old. Someone had completely carved off his face and cut off his fingertips. Someone really didn’t want him to be identified. Of course, for the purpose of teaching dentistry students, he was of no use.
“But I have to tell you that the most difficult time came four years ago when one of my brothers-in-law died suddenly and unexpectedly. He was only 33 years old. He had a heart attack. I was very close to him. I loved him. He was like my own brother. Before he died, I was always enthusiastic about doing dissection, teaching anatomy to my students, sharing my knowledge with them. But after my brother-in-law died, for several months, it was very hard for me to do dissection. We get so many young men. Whenever I saw a cadaver, I saw my brother-in-law. So the emotions kept coming up. I wished I could avoid dissection. After a few months, the emotion went away.”
I asked Dr. Martínez if his work with cadavers had changed how he thought about his own mortality.
“As a very young person I familiarized myself with the study of religion, particularly Eastern religion. I think people come up with fantastic answers to their questions about life. Like reincarnation, for example. We now know from science, from the study of genetics, that each human individual is unique. I don’t think anything like a personality, or a soul, survives after death. To the extent that we do survive in our children and grandchildren, it’s only in tiny bits and pieces. A smile. A way of laughing. A certain color of hair. But do I survive? The spirit that animates this body that you see? I don’t think so.
“I think the body is a vehicle. And like all vehicles, the better you take care of it, the longer it will last. The less you expose it to risk, the longer it will last. Graveyards are like junkyards. I think the metaphor is accurate. Sometimes, when a car breaks down, you can take a part from it and use it to repair another car. Just the same way you can take a part from one human body and use it to help another. From my studies, from all the cadavers I’ve seen and dissected, nothing has convinced me otherwise. I think this life is all that there is.
“My students tell me, year after year, that human dissection was a different experience from what they expected it to be. They say they thought it would be more gross, more disgusting. They thought the smell would be unbearable. But in the end, they tell me that what they learn and feel is compassion. They feel sorry for this body in front of them.
“It really is a big deal for my students. They are like virgins in many different ways. For most of them, this is the first time that they confront death in an undisguised way. This isn’t like seeing a body in a mortuary with all the clothes and makeup. Not only are they confronting death, but they’re also confronting human sexuality. All cadavers are naked. For the young, sexuality is very important. But here you have this body, male or female, and its sexual organs are sometimes exposed. For some of my students, this is the first time they’ve seen the naked body of the opposite sex. But no one makes a big deal of it. We’re learning about human anatomy. We’re learning to be objective. Certainly, the sexual organs are there, but we’re not paying attention to them. They’re not what we’re interested in. They’re just one other fact, one other aspect, of the human body.”
Dr. Martínez finished his manta ray tacos. I finished my orange soda. He drove me back to the yellow parking garage beside his clinic. Along the way he talked to me about his brother-in-law, the one who died four years ago when only 33 years old. He described his brother-in-law’s personality. He told me how hard his brother-in-law had worked, building a small print shop into a large, profitable business. Dr. Martínez talked about his sister, the widow, and her two daughters. He talked about how difficult their lives had been in the aftermath of his brother-in-law’s death. While Dr. Martínez spoke, my mind wandered.
When I saw my brother’s body in the south Oregon mortuary, my knees buckled. The funeral director helped me to my feet. My brother’s body was still wrapped in the white plastic bag in which the county coroner had delivered him. I wouldn’t touch his face. I touched his white-plastic–covered shoulder. His flesh felt cold and dense. I said, “It’s like those half-frozen turkeys you buy for Thanksgiving.”
On the small plane that took me from that small Oregon town, I looked out the window. Southern Oregon appeared vast. The sky, the distance from plane to ground below, magnified my sense of the world’s hugeness. Between that immense space and my brother’s cold body, I couldn’t imagine his soul. That something of him remained. That individual death in some broader sense matters.
“You’re wrong,” Dr. Martínez said when I told him what I’d been thinking. “The dead teach us. Every time you get medical care. Every time someone has something as simple as a root canal. Or when a child falls down and gets stitches in his chin. Or when you have a tooth pulled. Or when someone has major surgery. All the knowledge of how to do that came from somewhere. Doctors, dentists, surgeons don’t have to guess about what they’re doing. Where to cut. How to cut. How to suture. Where to inject and why. All that knowledge comes from the study of human anatomy. All that knowledge comes from human dissection, from studying the bodies of the dead. That’s all knowledge the dead have given the world. Most people probably aren’t aware of where basic medical knowledge comes from. The dead leave us information. Every time we receive any kind of medical care, we should be grateful to the dead.”
Here's something you might be interested in.
A visit to a Tijuana morgue
Baja anatomy professor: My students learn compassion.
A visit to a Tijuana morgue
Baja anatomy professor: My students learn compassion.
Dr. Luis Antonio Martínez and student. “Every week, while I’m driving to the university to do a dissection, I apologize to the people whose bodies we use."
"Doctors, dentists, surgeons don’t have to guess about what they’re doing. Where to cut. How to cut. How to suture. All that knowledge comes from human dissection, from studying the bodies of the dead."
Not long after my brother died and was buried in Oregon, I found myself in the depósito de cadáveres, or morgue, at Tijuana’s Autonomous University of Baja California. My hand rested on the handle of a large walk-in refrigerator. I wasn’t sure what I’d see inside.
Earlier in the day I attended a one-hour lecture given by Dr. Luis Antonio Martínez, a dental surgeon who teaches anatomy to students at the university’s dentistry school. His lecture was attended by 20 first-year students, of whom only 2 were male. Dr. Martínez was preparing his students for their first cadaver dissection. On the blackboard he drew a simple human face — ears, eyes, nose, mouth, chin.
“Next week you will first make a straight, horizontal, seven-centimeter incision two centimeters below the lip.”
The students, all in their early 20s, copied Dr. Martínez’s drawing of a face and his instructions into their notebooks. Dr. Martínez described how the students were to make three shallow incisions into the cadaver’s chin.
“Then you will take the top left corner of this trapezoid in your clamps and, inserting your scalpel at a 45-degree angle into the incision, begin carefully to cut, separating the skin from the tissue beneath.
“As you cut and pull away the skin, you will first see fat, which is yellow. You may also see muscle tissue, which, depending on the freshness of the cadaver, will be either deep pink or light brown.”
The young woman sitting next to me shuddered but didn’t look up. She wrote in her notebook “muscle tissue, deep pink, light brown.” Her fingernails were painted glittery red.
Dr. Martínez went on to describe three muscles his students would reveal beneath the skin and fat.
“And at the end of the dissection, I will show you why dissection is important. I will show you the precise points you will need to inject in order to anesthetize either the right or left front corner of the mouth. You’re going to see exactly where these points are, between the first and second bicuspid. When you work with patients, you won’t be able to see these points beneath the tissue. You will have to visualize them in your mind. By dissection, you will have a clear picture of where they are.”
Dr. Martínez, in khakis and pressed white shirt, his complexion fair, his skin unwrinkled, his thick dark hair combed straight back, didn’t look much older than the students he lectured. He is a 33-year-old father of three who, in addition to lecturing at the university two days each week, owns and runs two dental clinics. On a busy day like a Saturday, each of his clinics may see as many as 20 patients.
“I don’t have to teach,” Dr. Martínez told me. “But I love to teach. I like being around young people, their energy. When you’re my students’ age, you have everything to look forward to. You have all these dreams for your future. You get older, things change. Not long ago I was thinking about this, and I realized, ‘Hey, that future I used to dream about when I was young — I’m living that future now!’ ”
Dr. Martínez has been teaching anatomy at the university since he was 26 years old.
“You may notice that there are very few boys in my class. In Mexico, boys want to be doctors, not dentists. Boys have this idea that dentistry is delicate work, feminine work. It’s an entirely wrong idea. But I was like that. When I first went to university, I wanted to be a doctor. I had almost completed my first year of medical school when my grandmother was diagnosed with uterine cancer. My father wanted to do whatever was necessary to help her. He told me, ‘Son, the next year or so is going to be financially difficult for our family. I’m afraid you’re going to have to quit school for a while and get a job.’
“I went to San Diego and got a job as a waiter at Anthony’s. I loved it. On a good night, I could make $100 in tips. And they had jazz. That’s where I learned to love jazz. But my poor grandmother. The family spent over $120,000 on getting her the best medical care, on making sure she stayed in the best hospitals. But in the end, no matter how hard we tried, nothing could save her.
“When I went back to school, it was too late to enroll in the medical school’s second-year program. I would have had to wait another year. Professors on the dentistry school faculty said, ‘Come on! Study with us! You can start right away.’ I enrolled in the dentistry school, and I loved it immediately. I especially loved being able to continue the study of human anatomy.
“Even when I was a child, I was fascinated with the human body. I remember I saw the movie Frankenstein, and it was just amazing. The idea of a human body having different working parts, like a machine. I wondered how the body worked. I wanted to know how it was put together.
“From the very first time I participated in dissecting a cadaver, in the year I spent in medical school, I was overwhelmed by what a tremendous privilege it was to be able to examine the human body and learn in a very precise, detailed way how it worked. It’s really an honor to have that opportunity.
“When I finished dentistry school, I had done so well in anatomy that my professors asked me to take an additional two-year course of study in the subject so I’d be able to teach it. They felt that students of general dentistry, and not just dental surgeons, should have the opportunity to do dissection. So, anatomy is all I did for two years. Anatomy and dissection. And then I started to teach, which was a little strange because I was only a few years older than many of my students. I had to work hard to gain their respect. I had to show them, in a careful, thoughtful way, that I knew what I was talking about, that I was competent.”
On the afternoon Dr. Martínez and I met to talk, after he’d given his lecture on chin dissection, we sipped icy Cokes outside the university’s food court. Inside, students lined up before franchises for pizza, hamburgers, Chinese food, Mexican food, health food. Dr. Martínez explained to me that general dentistry students at the university paid around $160 in tuition per semester and that a degree in general dentistry usually took five years, or ten semesters, to complete. After the students graduate, the government requires that they spend one year practicing at a government-run clinic. He went on to tell me that in their first semester, the students study general anatomy, and in their second semester, descriptive anatomy of the head and neck, and then topographic anatomy of the head and neck by dissection. Dr. Martínez invited me to attend on the following Tuesday his class’s first cadaver dissection. A hot, dry wind was blowing from the northeast across the campus. My eyes watered and my mouth was dry. I asked if I might first see the morgue.
“Of course,” he said. “I understand. It’s best to approach these things little by little.”
He led me across campus to a low-slung, recently built structure with many windows set high in its beige walls. He led me into the immaculate white-tiled dissection room. He showed me the six waist-high, white-tiled dissection tables, each equipped with a water hose and a shiny stainless steel drain. In the northwest corner of the room, the walk-in refrigerator hummed.
“I don’t know how many we have today,” Dr. Martínez said, gesturing to the refrigerator. “If you want to look inside, you may.”
The day after my brother died, I went to the small Oregon town where he’d lived. I saw his body at the mortuary. He’d just been delivered from the coroner. I knew in my mind that he was dead. The mortician opened the door to the room where my brother lay. I saw my brother’s body. My knees gave out from under me.
At the university’s morgue, with Dr. Martínez watching, I opened the walk-in refrigerator. Cold air poured out. The refrigerator’s interior was dark. My eyes took several seconds to adjust. I saw three bodies lying on white gurneys. Blood-spattered muslin sheets covered the bodies. The air smelled of old blood.
Dr. Martínez asked, “So, do you think you’ll be able to attend our first dissection?”
“I think I’ll be fine,” I said.
“I apologize to them.” Dr. Martínez took me by the elbow. “Every week, while I’m driving to the university to do a dissection, I apologize to the people whose bodies we use. It’s not really a prayer. It’s just something I say in my mind. An apology for what we do.”
Greek religion prohibited the desecration of corpses. But it was the Greeks who were the first to take a scientific interest in human anatomy. By the Sixth Century BCE, the Greek treatment of disease had moved away from magic and spells, and the philosopher Alcmaeon conducted the first recorded attempts at human dissection, allowing him to discover, for example, the difference between arteries and veins. Later, Plato and Aristotle taught that body and soul were separate. This notion that the body was only a shell meant that cutting on a cadaver mattered little and helped assuage the public’s disgust at the practice. By 237 BCE Herophilus of Chalcedon, a follower of Hippocrates, established the world’s first school of anatomy in Alexandria, Egypt. But people remained uncomfortable with human dissection. The advent of Christianity and the doctrine of bodily resurrection gave further reason to the public’s discomfort. Whether the Catholic Church ever officially prohibited human dissection is unclear. Some medical histories contend that the Church banned the practice. The National Catholic Bioethics Center in Boston and the Catholic Encyclopedia assert that the Church never banned the practice, and they cite numerous instances of medieval scientists in Catholic countries who conducted human dissection without Church interference.
Two centuries after Martin Luther’s death, physicians throughout Western Europe knew that without dissecting cadavers, the systematic study of human anatomy was impossible. So began what some medical historians have called the “great cadaver shortage.”
The 18th Century witnessed scenes of people scrambling to steal corpses and sell them to physicians. The bodies of the anonymous poor were always up for grabs. In London, people fought over the bodies of executed criminals. The demand for cadavers was so great that some physicians resorted to grave robbing. Public sympathy for this trend was also in short supply. In 1788, 5000 New Yorkers rioted for three days after they learned that medical students at the Hospital of the City of New York were dissecting bodies stolen from a local graveyard. And today there are professors of literature who believe that this anger, fear, and suspicion were so pervasive that they played in Mary Shelley’s imagination when in 1818 she wrote Frankenstein.
A hot, dry wind was blowing on the early afternoon Dr. Martínez and his students met at the university morgue for the first dissection. We gathered in an anteroom where we put on gauzy blue surgical gowns, surgical masks, latex gloves, and blue surgical booties. A few of the girls giggled. Dr. Martínez joked with the students about how they looked in their surgical garb, about how they struggled to get the tight gloves over their sweaty fingers.
“I try to keep it light,” he later told me. “The first time is difficult.”
We pushed through the swinging doors into the dissection room. Dr. Martínez stood before us and clapped his gloved hands together.
“This isn’t a surgical setting, but I want you to behave as though it were. Once your hands touch anything in this room, your gloves are no longer sterile. Be careful not to rub your eyes or touch your mouths. Be conscious of where your hands are and what they’re doing.”
He asked two students to enter the walk-in refrigerator and wheel out the cadaver on the far left. Four young women darted to a bench on the dissection room’s far side, where they sat with their hands wedged under their thighs. Dr. Martínez pretended not to notice.
“You can’t play into the students’ fears,” he later told me. “You can’t create a fearful situation. I know a story of one professor who taught at another university, who was a very religious man and who was very nervous about doing human dissection. He would sweat. He would shake. He communicated his discomfort to his students. Some of them fainted. After one dissection, while he was closing an incision, he pricked his finger with the needle. A month or so later, he developed a small tumor in his finger right where he had pricked himself. He had the tumor removed. A few months later, the tumor reappeared. Again the tumor was removed. When the tumor was analyzed, it was determined that the tumor was somatic in origin. In other words, the professor was so nervous about doing human dissection, he was so worried about it, that his body had actually produced these tumors in his finger.”
When the students wheeled the cadaver into the dissection room, everyone grew quiet. Dr. Martínez and I each gripped two corners of the sheet in which the cadaver was wrapped and, grunting, lifted the body from gurney onto dissection table. Dr. Martínez pulled back the sheet to reveal the cadaver’s face: a dark-skinned young man with a head of thick, long black hair. His congealed eyes were half-open, his pupils were dime-size. He had stubble on his cheeks and chin, and, beside his left nostril, a small crusty purplish hole.
Dr. Martínez bent to examine the wound. “He was probably shot with a .38.”
“He looks so peaceful,” one of the students said.
“He probably didn’t die immediately,” Dr. Martínez said. “From his relaxed expression, I’m guessing it took him several minutes.”
One of the students, a young man, volunteered to play the role of surgeon. He took a black marking pen and drew the required trapezoid on the cadaver’s chin. Taking his scalpel, he started to cut, following the outline. Two girls seated on the bench wandered over to watch. One reached out to touch the cadaver’s shoulder.
“He’s cold,” she said. “And hard.”
When the three incisions were completed, the young surgeon folded back the skin.
“The yellow tissue is fat,” Dr. Martínez said. “I want you to remove it so you can see the three muscles I told you about.”
And the young surgeon, with tweezers and scalpel, started removing the yellowish pea-size globules. With delicacy he placed them on a pink surgical napkin that another student had draped across the cadaver’s naked brown chest. When the three muscles were revealed, Dr. Martínez asked the young surgeon to scrape them from the jawbone. “I want to show you the small hole in the jaw from which the nerve I told you about emerges.”
I could hear the sound of blade scraping bone. I examined the dead man’s feet.
“Notice his toenails,” Dr. Martínez told me. “They’re infected with fungus. We see that often in the cadavers we get. Many are migrants to Tijuana from rural southern Mexico, where people wear sandals and their feet have a lot of contact with soil. You can also tell he wore sandals from the calluses on the soles of his feet.”
The cadaver’s toe tag said he was an unidentified male, 25 to 30 years old, and that he’d been found on February 19, 2002, in Sanchez Díaz, a Tijuana neighborhood Dr. Martínez described as “violent.”
“Many bodies are found there. Drugs. Drug dealing. These people come up from the south to find work in Tijuana or cross into America, and they get mixed up in drugs.
“Fifteen years ago in Tijuana, we didn’t have enough cadavers for our medical students. Sometimes UCSD would send us some. Now everything has changed. The drug cartels. Thousands of migrants from the south. Tijuana has become so violent, we have plenty of cadavers. This is something very new in our city’s history.”
Sixteenth-century Spaniards brought the practice of human dissection to Mexico. Dr. Frank Gonzalez-Crussi, former head of pathology at the Children’s Memorial Hospital in Chicago and professor emeritus at Northwestern University, explained to me how this happened.
“The exact date is unclear. I’m guessing it was in the late 1500s, after the Conquest was completed. There was an outbreak of bubonic plague in Mexico City, and Spanish physicians, who’d arrived with the Conquistadors, dissected several plague victims at the Hospital de Jesús in Mexico City. That is the first known instance of scientific dissection in Mexico.
“What is remarkable about this is that we know that the Aztecs for centuries practiced human sacrifice. There’s some debate about the actual numbers of human sacrifices — hundreds, thousands, ten of thousands. We do know that they sacrificed at least hundreds of people. The Aztec priests would cut open the victim’s chest and offer his heart to the god Huitzilopochtli. What is interesting is that these priests, who had no qualms about cutting open a human body, showed no interest in the body’s organs, how the body was put together, how it worked. Despite all the many great achievements of Aztec civilization, in architecture and astronomy, the Aztecs took no interest in human anatomy. There’s no historical evidence that they ever made any attempt at all to study human anatomy.
“They didn’t see the human body in the same way as the Spaniards did. And this is a very important point to understand. Cultures literally see things in different ways. When the Aztecs opened a body, they didn’t see it as a kind of machine that had different working parts. For them, the body had a mystical significance.”
What is remarkable about Gonzalez-Crussi is that he is an immigrant from a poor Mexico City family who became, according to those who’ve reviewed his books, “America’s most beautifully eloquent writer on the subjects of pathology and human anatomy.” He’s authored seven books. He writes articles for the New Yorker. His most recent work, There Is a World Elsewhere, a memoir published in 1998, received excellent reviews in the Washington Post, the New York Times Book Review, and the Chicago Tribune. In 2001 he was named a Guggenheim Fellow and used the grant to complete his eighth book, “a book about birth. I began with a book about death and have written often about death, and now I’ve come full circle.
“Even as a child I knew I wanted to write, but I grew up in a proletarian neighborhood where wanting to be a writer could be only a kind of dream. I describe where I grew up in There Is a World Elsewhere. By the time I finished medical school in Mexico City and came to the States to complete my studies, I was absorbed in my career. Medicine is all-consuming. It requires not only enormous energy, but to move further, to make your way in the discipline, not to mention becoming a professor, takes up most of your life. When I was in my 50s, I decided it was time to write. I decided, ‘It’s now or never.’
“And I wrote about what I knew. Pathology. Human anatomy. Death. And I perhaps thought I could write about these things in a literary way because I grew up in Mexico, and there is a difference between the ways Mexicans and Americans regard death. I grew up with the Day of the Dead — I even ultimately wrote a book about it. Although my family didn’t make a shrine, or ofrenda, for the Day of the Dead, our neighbors certainly did. And there was this sense in Mexico that the dead are present with us. We don’t absent them. We want to keep in conversation with them. The familiarity with death is a little more in the air in Mexico than it is here in the United States.
“When I first arrived in America I was clearly told that death was something one didn’t discuss in ‘polite society.’ One colleague told me that discussing death or pathology in a social setting was like discussing pornography. It simply wasn’t done. Things have, of course, changed somewhat, but when I first got here, discussing death anywhere outside a clinical setting was taboo.
“Of course, the great irony of this was that the United States had become preeminent in the world not only for the study of pathology and human anatomy, but for medical science in general. This was a huge change. Before World War II, Germany had been the world’s great center for the systematic study of human anatomy. Even into the late 19th Century, the systematic study of human anatomy hadn’t truly evolved as a discipline at the University of Mexico City. Mexican doctors who wanted to study pathology and human dissection went to Germany, or to Austria, which was also very strong in those fields.
“There are some people who may disagree with me, but the systematic study of human anatomy didn’t truly become a discipline in Mexico until the 1920s, when President Lázaro Cárdenas accepted many Spanish refugees who were fleeing Franco. In many instances, these people were la crème de la crème of the Spanish intelligentsia. One of these refugees, Isaac Costero, who’d studied in Germany, really founded anatomical pathology as a discipline at the University of Mexico City.”
I asked Dr. Gonzalez-Crussi if, after his many years as a pathologist, he’d ever grown used to human dissection.
“No. Not even after many years. You do develop some tolerance, but no, it never becomes just a job. I suppose there are some callous people for whom the practice might become routine. In some ways the spectacle of autopsy is such that it may lead some people to think of the body only as a machine. Most doctors are inspired by that kind of philosophy. They may tell you that the human body is a wonderful machine, but it’s still a machine. The workings of a machine may be more or less completely understood.
“That we are animal, that we are mechanical, I have no doubt. But it can’t be reduced to that and nothing else. We may completely understand the anatomy of the human brain, but we can’t explain what composes a symphony in the brain of a composer. Thoughts cannot be explained only by mechanism.
“And this is part of the mystery revealed by the spectacle of the cadaver. This is why human dissection is so impressive. It underscores all these questions. And, most significantly, when confronted with a cadaver, you can’t deny the reality of all it implies. The cadaver points to the path which all of us without exception will follow.”
I asked Dr. Gonzalez-Crussi whether he’d ever gotten used to his work because two weeks after the first dissection, I returned again to Tijuana to attend another. Dr. Martínez had explained to me that the purpose of the first dissection was to acquaint his students with the process itself.
“I want them to get over their fears, their nervousness, so they can actually start seeing the body in an objective, scientific way. I don’t want them ever to learn to disrespect the cadaver or treat it casually. I’ve suspended students even for making unnecessary incisions on cadavers. But I want them to see the human body objectively. In order to work on living people, you have to. That’s why physicians and dentists almost never treat family members. It’s almost impossible to look objectively at the body of someone you love. When you’re dealing with someone you love, it immediately becomes subjective. I’ve tried a couple of times to work on my children’s teeth, but it was impossible. If I hurt them, for example, when I gave them an injection, and they started to cry, it was unbearable for me. I’d hurt my child. They’d start crying, and I’d almost feel like crying myself.”
The second cadaver was that of a strong, handsome, broad-shouldered young man. His toe tag said he was unidentified, between 19 and 22 years of age, and that, on February 2, 2002, he’d been hit by a car while crossing the old road to Tecate. He was so heavy that we couldn’t lift him from his gurney.
Dr. Martínez pulled back the sheet. The young man’s right side, from armpit to hip, was covered with dark bruises and deep lacerations. His right shin, just below the knee, had been fractured completely. Broken bone poked through skin, revealing sinew and muscle. Below the fracture, the leg could be moved back and forth, as if it swung on a hinge. The young man’s brown belly was distended. Dr. Martínez explained that he’d suffered massive internal injuries. And that was why, Dr. Martínez said, the cadaver had a high smell.
The odor was cloying. I could smell it even through my surgical mask — a very strong meaty odor. Unpleasant. Something that couldn’t be gotten used to. Hours after I left the dissection, had driven home from Tijuana, showered, brushed my teeth, changed clothes, settled in for the night, the smell stayed with me. (A doctor friend later told me, “The trick is to smear a little Vicks VapoRub on your upper lip or on the inside of your surgical mask. It helps.” Dr. Martínez later told me, “I always drink a lot of coffee before a dissection, so when I’m breathing in my surgical mask, the only thing I smell is coffee.”)
Perhaps it was because of and not despite this odor, and the sheer size of the cadaver, that the reality of the human body as flesh was clearer to me. Witnessing the second dissection was easier. Dr. Martínez’s students, too, were more at ease. No one ran off to sit on a bench. Everyone gathered around the gurney. A young woman volunteered to play the role of surgeon. She began to make the same trapezoid-shaped incision on the cadaver’s chin.
“This time,” Dr. Martínez said, “we’re going to proceed more carefully, more slowly, as if we were operating on a living patient.”
The young woman was very precise. She took her time. While she worked I asked Dr. Martínez if he ever wondered about the lives of the people his students dissected.
“It’s inevitable. They’re human beings. And you wonder what their story was, what brought them to the dissection table. Every now and then we get a young man with the words ‘Mara Salvatrucha’ tattooed across his chest or back. From watching the news, I learned that this was the name of a Salvadoran gang that preys on people crossing the Mexican-Guatemalan border. But why do they end up dead here, in Tijuana? Over the years, I’ve seen certain patterns emerge. We get more suicides during the winter when people become depressed and drink more. We get more women during the summer months, when there are more parties, when men go out drinking and looking for women. We get a lot of prostitutes. Women from the interior of Mexico who come north looking for work, and the only work they can find is prostitution. Some of them end up dead. Found strangled or smothered in a hotel room. I remember one woman in particular. She had been strangled. She had stretch marks that suggested recent pregnancy. And her breasts where swollen, as if she’d been nursing. She had, I noticed, track marks on her arms. She’d been using drugs. And I couldn’t stop thinking about her. A child, somewhere, had lost his mother.”
When the young woman had completed her dissection of the cadaver’s chin, had peeled back the skin, removed the fat and muscle, Dr. Martínez took charge. He pointed to a small hole in the cadaver’s chin from which emerged a thin, pearly-white strand of tissue.
With a pair of tweezers Dr. Martínez pulled at the strand, what Gray’s Anatomy identifies as the mental nerve. (“Mental” in this case coming from the Latin mentum, relating to chin, and not from mens, relating to the mind.)
“This is the nerve I told you about. And it’s exactly right where I told you it would be, directly below the first and second bicuspid.”
Dr. Martínez pulled back the cadaver’s lip and inserted a probe between the gum and lip, beneath the first and second bicuspid. He poked the probe through the tissue, and it emerged precisely at the mental nerve’s base.
“You see, this is where you must insert your needle when you need to anaesthetize this part of the mouth. Now that you’ve seen where the nerve is located, you can have a clear picture in your mind when you’re working on a patient. This is why dissection is so important.”
In Mexico, it can also be lethal. There are Mexicans who, for reasons other than religious or moral, prefer that the dead remain untouched. In Mexico, forensic pathology can be dangerous.
In an idle moment, Dr. Martínez told me about Dr. Irma Rodríguez, who, until July 2001, worked as medical examiner for Ciudad Juárez, just across the border from El Paso.
“There aren’t a lot of people in Mexico who want to study forensic medicine or dentistry. At the university here, they only offer a six-month course in those subjects every now and then. I took a course in forensic dentistry because it interested me. I do it only as a sort of a hobby. Maybe two or three times a year, a family needs a body to be identified and they’ll have dental records. It’s actually not very complicated to do.
“But Dr. Irma Rodríguez was involved in identifying bodies found in mass graves that had been discovered in ranches outside Ciudad Juárez. Everyone knew that the drug cartels were involved. Everyone knew that these mass graves existed. Everyone knew that the authorities were aware of the mass graves. And everyone knew that the drug cartels didn’t want the bodies found in those mass graves to be identified. Dr. Rodríguez must be a very brave woman. As I said, few people in Mexico study forensic medicine.
“What happened in July of last year was that someone, it isn’t clear who, shot and killed Dr. Rodríguez’s husband and daughter. From what I understand, Dr. Rodríguez was away at the time, attending a conference in Mexico City. Dr. Rodríguez’s daughter was driving Dr. Rodríguez’s car. And there are some people who believe that the gunmen mistook the daughter for Dr. Rodríguez. The details aren’t clear. Someone wanted to send a message. Someone didn’t want the bodies in those mass graves to be identified. Someone wanted to send a message that Mexico wasn’t perhaps the best place to make a career in forensic dentistry or medicine, at least not in Ciudad Juárez.”
I was in the lobby of the Tijuana medical examiner’s office, Servicio Médico Forense de Tijuana, on the morning of April 11 — the morning after Tijuana’s chief of police, Carlos Otal, and 200 other law enforcement officers, were arrested by Mexican federal authorities. I was studying a sign posted in the lobby that said, We Respect Your Pain: We Accept Neither Gifts Nor Gratuities for Our Services, when several plainclothes officers walked in. They wore tailored shirts and snug Calvin Klein jeans and freshly polished boots. They had tucked guns under their waistbands. They were gossiping about the previous day’s scandal. It sounded as though Chief Carlos Otal, at the time of his arrest, reacted with less dignity than was expected from a public official confronted with a touchy situation.
“He screamed, ‘You’re treating me like a common criminal!’ ” one of the plainclothesmen said.
“He yelled, ‘Hey, be careful! You’re getting my pants dirty!’ when they were dragging him away.”
I was at Servicio Médico Forense de Tijuana on Boulevard Fundadores, just a block or so south of Happy Chicken restaurant, because I wanted to speak with the servicio’s director, Dr. Luz Vertila Ontiveros. But la doctora was late. I went outside the lobby for a cigarette. While I smoked, the wind blew a sheet of old newspaper at my feet, a page from the February 27, 2002, edition of El Mexicano.
An article entitled “One Shot to the Head” described the execution-style slaying of a 36-year-old man who lived in a Tijuana neighborhood called the Hills of Friendship. Another article described the arrests of four kidnappers who, in a residence near the intersection of Kiwi and Strawberry Streets, had held captive a woman named Nancy. Another article detailed how a group of six young men armed with high-power weapons had “with extreme violence” kidnapped a 40-year-old man. The group’s leader, the article said, “was presumed to have dedicated his life to the sale of drugs.”
Dr. Luz Vertila Ontiveros, a pretty and coquettish woman in a pristine lab coat, told me she oversees between 800 to 1000 autopsies each year.
“I can’t give you a more precise figure because it varies. I’ve been here for seven years, and each year the numbers have been different. What I can tell you is that we have a staff of nine forensic examiners and we receive the bodies of people who die unattended, outside a hospital or doctor’s care. We also receive the bodies of people who die in hospitals but who have no family. And we, of course, get the bodies of people who die of unnatural causes. Crime victims. Bodies that have been left somewhere.
“I’d estimate that between 10 and 20 percent of the bodies we receive are unidentified. We take their dental impressions, their fingerprints. We take pictures of them. By law we’re required to hold unidentified bodies for ten days. After that, we hand over our autopsy reports and identification materials to the state judicial office. Of those unidentified bodies, we send several every week to the university for dissection by medical and dentistry students. The bodies must be intact and in good condition. We clean and embalm them. We also test them for HIV. Only HIV-negative cadavers are sent to the university. The rest of the bodies are sent to a municipal cemetery and are buried in a common grave, as are the cadavers used at the university after the students are done studying them.”
I asked the doctor if she’d heard of Irma Rodríguez. She paused.
“Well, of course. Forensic medicine is a dangerous profession in Mexico. But, here, we’re left alone. We work for the city. We do our job. No one bothers us.”
Panteón Numero 11, Municipal Cemetery Number 11, is where Tijuana for the past two years has sent its unidentified dead for burial. (The ten other municipal cemeteries can no longer make room for them.) To get to Municipal Cemetery Number 11, you take the Via Rápida, or freeway, that runs from Zona Rio to the far southeast of Tijuana. The Via Rápida’s on-ramps are difficult to navigate and offer even the most skillful driver an intimation of mortality. On the afternoon I managed to get onto the Via Rápida, an old white pickup rumbled in front of me for many miles. In the back of the truck bounced four rusty drums. Written in big red block letters on the tailgate were the words Material Peligroso, Dangerous Material.
Municipal Cemetery Number 11 sits a mile or so behind Mount of Olives, a well-kept and privately owned cemetery for the city’s middle and upper classes. To get to Municipal Cemetery Number 11 you turn right at the Mount of Olives’ entrance and continue up a rocky and deeply rutted road.
“We serve the people” is what one of the municipal cemetery’s workers told me as he led me to where the unidentified are buried. “It costs maybe $50 for a family to bury someone here. It’s inexpensive and their family member can have a dignified grave.”
The unidentified rest at the bottom of a steep hill. A thin metal spike marks each common grave, each grave holding, I was told, 10 to 20 bodies. In this southeastern part of Tijuana, the hills are brown and barren. Across from the common graves, a hundred or so yards away, stand several ramshackle homes built by squatters. When the wind was right I could hear domestic noise from those homes — a woman calling for her children, a rooster crowing. Wild mustard glazes a gully that runs beside the common graves. Plastic Coke bottles, transistor batteries, an old hairbrush litter the earth covering the common graves.
Up the hill, people have surrounded many of the $50 graves with small white picket fences. Other families have provided not only small white picket fences but have also hauled patches of fresh sod to Municipal Cemetery Number 11 and planted them atop the graves. The headstones on these more elaborate $50 graves look like small houses, and they hold pictures of the deceased. From their perspective, the deceased stare out at a patch of green lawn surrounded by a white picket fence, the sort of view afforded by the living-room window of a suburban dream home.
Plastic flowers and bits of ribbon sometimes drift down to the common graves. If anyone has ever visited them, they’ve left no sign. I counted 118 thin metal spikes. There were probably more, but the air at the bottom of the hill was hot and oppressive, and small black flies worried my forearms and back of my neck. I made my way back up the hill. Two funerals were in progress. I could see another hearse making its way up the long, rocky, rutted road. A Popsicle salesman trundled his cart toward one of the funerals. Not far from the other funeral sat a little boy on an upturned blue bucket. He was selling plastic sacks of pork rinds to the mourners.
Dr. Martínez’s main office sits on Third Street in downtown Tijuana, between Constitución and Niños Héroes, at the entrance to a large yellow parking garage. I went to visit him at his office not long after I’d visited Municipal Cemetery Number 11. The news on my car radio that morning concerned troubles at the Los Angeles medical examiner’s office.
“I know there have been reports of rats gnawing at the bodies in our care,” an L.A. forensic examiner said. “But we’re really not talking about gnawing here. We’re talking about a full-on meal.”
I found Dr. Martínez in good spirits. He’d just learned that a team of Cuban physicians was coming to the university to offer a certificate program in oral pathology.
“I’m going to take the course,” he told me. “The only thing is that you have to take the final exam in Havana. But, you know, that’s sort of my dream. To keep on learning. I think that if I work hard enough, someday, after my children are raised, that’s all I’ll do. I’ll take courses and maybe write a little.
“For the past two years I’ve been writing a textbook for dentistry students on head-and-neck dissection. Right now, they have to buy a general text on dissection that costs around $50. My book would cost only $6 or $7. And it’s written specifically for general dentistry students.
“I think it’s this kind of attention that makes our students the best in Mexico. Every year, there are seminars for dentistry students, and they take national exams. Every year our students have the highest scores. The quality of education here is very high. We have a close relationship with the dentistry school at UCSD. From them we learn about all the newest advances in American dentistry. They help us acquire the latest equipment. Our quality of care here is very high. I say this knowing that there are dentists in San Diego, in America, who tell people not to come to Tijuana for dental work. They say that we’re dirty. That we don’t sterilize our equipment. It’s sort of ridiculous. I have friends who work at certain dental clinics in San Diego, clinics that deal mostly with immigrants. My friends work as dental assistants. I hear horror stories.”
Dr. Martínez offered to take me for an early lunch at a fish taco restaurant near Guerrero Park. I accepted and when we arrived Dr. Martínez immediately ordered for himself tacos made of manta ray.
“I compartmentalize very well,” he said, shaking hot sauce onto his tacos. “I don’t let associations from one thing carry over to another. At home, I don’t talk about dentistry or dead people. At the clinic, I don’t talk about my personal life. I keep things separate. Right now, I can talk about my work at the university, and it wouldn’t bother me.”
I asked him if, after all these years, his work in dissection didn’t at times bother him.
“Several instances come to mind. I remember a couple, a boy and a girl, maybe 15 or 16 years old. This was maybe three years ago. They’d both been shot in the back of the head with a shotgun. From what I understand, when their bodies were found, they were still holding hands. They were in some gully. In some ravine. They’d been shot in the back of the head. Why?
“Two years ago, there was an eight-year-old boy. You know, one of the kids who just lives on the street. And he’d been stabbed. He died of multiple stab wounds to his abdomen. He was just one of those kids that we now have in Tijuana that just lives in the streets. No one claimed him. He was unidentified. I have children of my own. And there was this little boy. I sort of cuddled his body. I spoke to him gently because, I thought, maybe no one in his life had ever cuddled him or spoken to him gently.
“And of course I didn’t use him for dissection. I can’t. I understand that for the medical school it’s very important that they learn pediatric anatomy. That’s how they learn to care for children. A child’s anatomy is so different from that of an adult. But I’ve never been able to use a child for dissection. A year or so ago there was an 11-year-old girl. She was raped and strangled. You could still see the finger marks on her throat. And so, no. No. To cut her face? No.
“And not long ago they sent us a cadaver with no face. It was a young male. Maybe 20 years old. Someone had completely carved off his face and cut off his fingertips. Someone really didn’t want him to be identified. Of course, for the purpose of teaching dentistry students, he was of no use.
“But I have to tell you that the most difficult time came four years ago when one of my brothers-in-law died suddenly and unexpectedly. He was only 33 years old. He had a heart attack. I was very close to him. I loved him. He was like my own brother. Before he died, I was always enthusiastic about doing dissection, teaching anatomy to my students, sharing my knowledge with them. But after my brother-in-law died, for several months, it was very hard for me to do dissection. We get so many young men. Whenever I saw a cadaver, I saw my brother-in-law. So the emotions kept coming up. I wished I could avoid dissection. After a few months, the emotion went away.”
I asked Dr. Martínez if his work with cadavers had changed how he thought about his own mortality.
“As a very young person I familiarized myself with the study of religion, particularly Eastern religion. I think people come up with fantastic answers to their questions about life. Like reincarnation, for example. We now know from science, from the study of genetics, that each human individual is unique. I don’t think anything like a personality, or a soul, survives after death. To the extent that we do survive in our children and grandchildren, it’s only in tiny bits and pieces. A smile. A way of laughing. A certain color of hair. But do I survive? The spirit that animates this body that you see? I don’t think so.
“I think the body is a vehicle. And like all vehicles, the better you take care of it, the longer it will last. The less you expose it to risk, the longer it will last. Graveyards are like junkyards. I think the metaphor is accurate. Sometimes, when a car breaks down, you can take a part from it and use it to repair another car. Just the same way you can take a part from one human body and use it to help another. From my studies, from all the cadavers I’ve seen and dissected, nothing has convinced me otherwise. I think this life is all that there is.
“My students tell me, year after year, that human dissection was a different experience from what they expected it to be. They say they thought it would be more gross, more disgusting. They thought the smell would be unbearable. But in the end, they tell me that what they learn and feel is compassion. They feel sorry for this body in front of them.
“It really is a big deal for my students. They are like virgins in many different ways. For most of them, this is the first time that they confront death in an undisguised way. This isn’t like seeing a body in a mortuary with all the clothes and makeup. Not only are they confronting death, but they’re also confronting human sexuality. All cadavers are naked. For the young, sexuality is very important. But here you have this body, male or female, and its sexual organs are sometimes exposed. For some of my students, this is the first time they’ve seen the naked body of the opposite sex. But no one makes a big deal of it. We’re learning about human anatomy. We’re learning to be objective. Certainly, the sexual organs are there, but we’re not paying attention to them. They’re not what we’re interested in. They’re just one other fact, one other aspect, of the human body.”
Dr. Martínez finished his manta ray tacos. I finished my orange soda. He drove me back to the yellow parking garage beside his clinic. Along the way he talked to me about his brother-in-law, the one who died four years ago when only 33 years old. He described his brother-in-law’s personality. He told me how hard his brother-in-law had worked, building a small print shop into a large, profitable business. Dr. Martínez talked about his sister, the widow, and her two daughters. He talked about how difficult their lives had been in the aftermath of his brother-in-law’s death. While Dr. Martínez spoke, my mind wandered.
When I saw my brother’s body in the south Oregon mortuary, my knees buckled. The funeral director helped me to my feet. My brother’s body was still wrapped in the white plastic bag in which the county coroner had delivered him. I wouldn’t touch his face. I touched his white-plastic–covered shoulder. His flesh felt cold and dense. I said, “It’s like those half-frozen turkeys you buy for Thanksgiving.”
On the small plane that took me from that small Oregon town, I looked out the window. Southern Oregon appeared vast. The sky, the distance from plane to ground below, magnified my sense of the world’s hugeness. Between that immense space and my brother’s cold body, I couldn’t imagine his soul. That something of him remained. That individual death in some broader sense matters.
“You’re wrong,” Dr. Martínez said when I told him what I’d been thinking. “The dead teach us. Every time you get medical care. Every time someone has something as simple as a root canal. Or when a child falls down and gets stitches in his chin. Or when you have a tooth pulled. Or when someone has major surgery. All the knowledge of how to do that came from somewhere. Doctors, dentists, surgeons don’t have to guess about what they’re doing. Where to cut. How to cut. How to suture. Where to inject and why. All that knowledge comes from the study of human anatomy. All that knowledge comes from human dissection, from studying the bodies of the dead. That’s all knowledge the dead have given the world. Most people probably aren’t aware of where basic medical knowledge comes from. The dead leave us information. Every time we receive any kind of medical care, we should be grateful to the dead.”
Comments