{kind=link}
Here's something you might be interested in.
Ask a Hipster — Advice you didn't know you needed
Big Screen — Movie commentary
Blurt — Music's inside track
Booze News — San Diego spirits
Classical Music — Immortal beauty
Classifieds — Free and easy
Close to Home — What it’s like on the street where you live
Cover Stories — Front-page features
Drinks All Around — Bartenders' drink recipes
Excerpts — Literary and spiritual excerpts
Feast! — Food & drink reviews
Feature Stories — Local news & stories
Fishing Report — What’s getting hooked from ship and shore
From the Archives — Spotlight on the past
Golden Dreams — Talk of the town
The Gonzo Report — Making the musical scene, or at least reporting from it
Letters — Our inbox
Movies@Home — Local movie buffs share favorites
Movie Reviews — Our critics' picks and pans
Musician Interviews — Up close with local artists
Neighborhood News from Stringers — Hyperlocal news
News Ticker — News & politics
Obermeyer — San Diego politics illustrated
Outdoors — Weekly changes in flora and fauna
Overheard in San Diego — Eavesdropping illustrated
Poetry — The old and the new
Reader Travel — Travel section built by travelers
Reading — The hunt for intellectuals
Roam-O-Rama — SoCal's best hiking/biking trails
San Diego Beer — Inside San Diego suds
SD on the QT — Almost factual news
Sheep and Goats — Places of worship
Special Issues — The best of
Street Style — San Diego streets have style
Surf Diego — Real stories from those braving the waves
Theater — On stage in San Diego this week
Tin Fork — Silver spoon alternative
Under the Radar — Matt Potter's undercover work
Unforgettable — Long-ago San Diego
Unreal Estate — San Diego's priciest pads
Your Week — Daily event picks
Why San Diego asthmatics won't take their meds
Breathless

Lynn Devine: “You want to feel as if you have someone who can rescue you."
THIS IS WHAT ONE KIND OF BAD ASTHMA ATTACK IS LIKE.
At half-past midnight on a November night in 1991, my stomach suddenly felt uneasy. This was hardly unusual. For the past month, barely a day had gone by without heartburn. I sat up in bed and groped around for the Rolaids. By the time I found them, my stomach was acidic, turbulent. I ate two. Within a few minutes my entire metabolism changed,
Michael Welch, one of the premier asthma physicians in the country.
My sinuses were swelling, stiffening, filling up, my ears and cheeks were getting hot, my spine and my chin itched. Everything was closing in around my throat and chest; I felt a frightening internal claustrophobia, a sense of metabolic urgency rapidly mounting toward panic.
Edward Vogel demonstrating alternate nostril breathing
I already knew this was no ordinary asthma attack. I had my first attack nearly 30 years before, and over the years I came to recognize several kinds of asthma. Most were a lighter or heavier wheeze that came on gradually, last thing at night, or more suddenly when shoveling snow in a heavy coat. They sounded like the word “asthma,” a sibilant rasp.
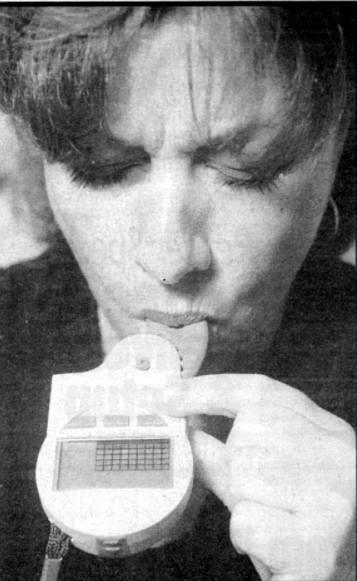
The Airwatch readings tell him how freely he is breathing at the moment.
Three times since I’d turned 30, though, something entirely different had happened; a sudden, overwhelming assault had stormed through my whole body, seizing my throat and suffocating me. This felt like one of those asthmas.
Tai-Nan Wang. “Alex no longer takes any medication at all, thanks to Dr. Wang."
I swung my legs over the side of the bed and put my palms on my knees in the classic asthma breathing position, wondering what the hell had brought on this attack. It felt as if I’d eaten something I was allergic to, what with the reaction throughout my whole body, the weird stomach.
Dr. Edward Golub suggests a different way of looking at asthma.
But what had I eaten? Fontina cheese and crackers; a bottle of Dos Equis and a bottle of Grolsch; pumpkin pie and ice cream — nothing I hadn’t had before. Rolaids? I’d been taking them for a decade. They didn’t contain aspirin, did they? Weren’t they just chalk?
Well, what about stress? Christ, what stress wasn’t I under? I was going through a divorce, I was teaching four classes at the university on top of my usual freelance writing— but could stress really cause an attack this bad?
I fumbled around on my night table and found a Primatene inhaler, the kind you see advertised on television with lackie Joyner-Kersee taking a quick hit, recovering in 15 seconds, and then sprinting to a gold medal. It’s an over-the-counter medication the doctors view askance, knowing its predilection for unfortunate cardiac side effects: raised blood pressure, even heart attacks. But my prescribed albuterol inhaler didn't seem to help much anymore; I suspected I was becoming allergic to the propellant — a disturbing thought. The Primatene seemed to work better, so my GP shrugged and said, “Sure. Give it a try.’’ I squeezed the Primatene and drew the spray in deeply.
For a few seconds I thought it had worked. But even as I breathed a little more easily, I felt the mounting urgency of the attack in the rest of my system. My sinuses were now completely solid and swelling further, pressing against my cheeks and eyes. My face, ears, and neck burned, and a desperate itch ran up and down my spine.
I had to get to some epinephrine. Also known as adrenaline, it was what I had been given when I was rushed to the hospital with my asthma emergency. Since then I had been trained to inject myself in the thigh and carried a kit (called Ana-Kit, short for anaphylaxis kit) around with me. Once, during a moderately severe attack, I had given myself a half-dose, just for practice, and it had worked fine: easy to inject, swift relief. I woke Barbara, my girlfriend. She had never seen a major asthma attack before; I knew that it would probably be more frightening for her than for me. From the outside, the sufferer of asthmatic anaphylaxis looks as if he is collapsing inwards, drowning in an invisible sea of himself. “In the car,” I said, trying to show calm, measuring my phrases to fit the amount of air that I could muster. “In the glove compartment. Is my epinephrine syringe. Please go and get it. Right away. Here are the keys.”
Alarmed, she dressed hurriedly and ran out.
The attack was mounting rapidly. By now I had two hearts, one in each ear. The effects of the Primatene had been overrun, and I felt my chest and throat tightening around my windpipe. My upper body had become panic, operating with a life and purpose of its own. I felt as if my intelligence had suddenly separated from a body gone amok and left alone and in charge, like the captain of a torpedoed ship with six deck-loads of passengers and crew milling around and beneath him, screaming, and the engines driving the ship straight down. But the epinephrine would stop all this. Everything would be all right as soon as the epinephrine arrived.
Barbara burst in with the kit, not the half-used Ana-Kit but an ostensibly more sophisticated tool I had been given since, an EpiPen syringe, commonly prescribed for those with potentially fatal bee-sting allergies. When I opened the tube, I saw that to my
surprise it didn’t look like a syringe but a large gray ballpoint without a nib. Press against thigh and hold in place for ten seconds. I did so. Nothing happened. I pressed my thumb against the butt-end; perhaps I had to push the needle in myself. Still nothing. How did this damn thing work? I jabbed it harder against my leg. There was a thudding noise, and I felt the needle ram into my muscle with not a stabbing pain, but that deep, unnerving thump that is the real sensation of a stab wound. I was startled — but at least the epinephrine was going in. Now things would be all right.
To be on the safe side, I waited 30 seconds before withdrawing the needle. As it came out I was surprised first at the length of it — no wonder they keep it retracted! — and then at the sudden rush of blood. This shouldn’t be happening! I cupped my hand under it, yelling for a paper towel. Three fat drops seeped between my fingers and spread into the white cotton rug. Next morning they would be the only visible signs of the night’s events.
Within a couple of minutes it became clear that the epinephrine wasn’t working. Had it all bled out? Had I developed a resistance to it? What the hell was going on?
Asthma feeds on panic; asthma is panic. I breathed from my diaphragm and calculated. The Primatene, unlike the albuterol inhalers, contains epinephrine — 0.3 mg per dose, I thought. I had just injected myself with another 1 mg. How much would it take? What would happen if I took too much?
This is the paradox of chronic illness. The patient grows around the disease, like an oak tree engulfing a barbed-wire fence in its trunk. My own habits and shortcomings probably perpetuate the condition; the asthma disappears under the bark of my character where I am least likely to look for it. The answer, it would seem, is to remain vigilant, to inform oneself of the latest research, the newest medicines — but such vigilance shades into hypochondria; and, more importantly, anxiety brings on asthma. Research suggests that those who worry most about asthma are probablv those who resort most swiftly to the inhaler; and there nothing so terrible as the sight of someone sucking on an inhaler every half-hour, a slave to his own salvation. Breathe slowly, I told mvself; think quickly.
It was an eerie, vertiginous feeling. I was confronting the normally unexamined mechanics of staying alive, like the clock face turning and staring at the movement in the case. What are the most vital functions? Breathing. Heartbeat. Brain activity. Of these only breathing is at all voluntary. The cardiac patient, sensing the onset of arrest, can't will his heart back to its measured beat, soothing it down from a frightening erratic fibrillation; he can’t rip open his chest and squeeze once a second, his life literally in his own hands. Only with breathing are we given the devil’s option, the chance to Keep ourselves going by force of will.
Barbara hovered around me, trying to stroke my neck, asking questions. My irritation rose like the flush in my skin. I did not need love; I needed competence. “In the kitchen,” I told her. “Opposite the sink. Top shelf. Ana-Kit. Orange plastic box. Rectangular. Under the sink. Bottle of alcohol. Get them both now.”
She found the half-used Ana-Kit and the alcohol. I’ve used the needle before, so it will have to be sterilized, reasoned my intelligence, pacing the bridge, though I had no idea whether dipping the needle in alcohol would kill all the germs or whether at this stage that even mattered. I dabbled it briefly, then jabbed it at my thigh. It bounced off. Maybe the needle had been blunted and wouldn’t work a second time? I pushed harder and it slid through the skin as if through linoleum. I gave myself another 0.5 mg of epinephrine. This, surely, would be enough.
I sat on the edge of the bed, naked, hauling in breath, bent over like a coal man hauling his sack. The epinephrine did not work.
I used to live near Accles & Pollock, in Worcestershire, England, the company that according to the Guinness Book of World Records made the thinnest tubing in the world at the time, its bore being a hundredth of an inch or so, more of a thread than a tube. That’s what my trachea felt like. I can get just enough air to survive if I don’t move or talk, if I can focus on the muscles in my throat and convince them not to contract still further. Even so, I realized I was better off than during my first major attack, in 1984, when that thread of a tube filled up with fluid, and I knew what it is like to drown.
I was dimly aware that Barbara was asking, “Shall I call an ambulance?’’ looking anxious. I nodded. My face felt stretched, like Edvard Munch’s screamer. I thought of an elderly woman I once knew who died slowly, losing touch with her surroundings, sinking in on herself, confused, muffled, protected from knowing what was happening as if the body released some hormone that made it all not matter very much. That’s how I want to die, I thought.
Anything but dying fully aware and in a panic.
My head had started aching. By now sharp pains shot through my back whenever I breathed in. Technically, asthma is caused by not being able to breathe out; patients have died with substantial amounts of air trapped in their lungs. It doesn’t feel that way to an asthmatic. Breathing in is inspiration, the grasp for the straw of air. Breathing in is the beginning of life, the first gulp as the diver reaches the surface. No asthmatic works to breathe out.
The fire crew arrived and flitted around like shadows—dark, unimportant, almost unreal. I’ve read that to an addict, nothing but his drug matters; and at this point I knew that this must be true in a literal sense: nothing but the drug has matter. Everything outside me was insubstantial, at most only a distraction, an irritation. Shades of people moved around the room, asking questions I couldn’t answer, murmuring to each other, their walkie-talkies crackling. The only person I wanted to see was the one with the cure, which would give him or her definition and meaning. For once I could see what Sartre meant, we are given not only purpose but existence by our acts. Barbara and the fire crew couldn’t help, so they vanished; I shrank further into myself and worked on giving myself existence by breathing.
At one point the panic rose like a wave and engulfed me. “Help me,” I croaked to one of the fire crew. He stared at me. He doesn’t know what to do, I thought. I shouldn’t have involved him. I turned back into the internal world, where I was needed and could be of some use.
The ambulance crew arrived. “Do you feel as if you’re going to pass out?” they asked. I worked up enough air to talk. “I feel. As if. I’m going to die.” That answer didn’t fit their criteria for an informative response, and at once it became clear that they couldn’t do anything to help me either. But at least we would be off to the ER, which was only a few minutes up the hill.
First, though, they had to get me out of the house. “Can you put your clothes on? Can you get into the chair?” they asked; and when I didn’t answer they thought I was being stubborn or I couldn’t understand them, and they repeated the questions several times. But in the sick man’s solipsistic wisdom, I knew better than they. The slightest movement, even talking, involved constricting some group of muscles, and every muscle was now connected to my chest, pressing on it. I had to plan every movement ahead, to imagine the most efficient, the most graceful way of doing it, then wait half a minute to relax as best I could, make the movement and collapse into myself afterward as my pulse shot up and my hearts pounded in my ears, my thread of air temporarily crushed. I felt like a dwarf— large head, barrel chest, puny arms, virtually nonexistent below the diaphragm. I had shrunk to all that mattered. It amazed me that when I finally half-stood, I was taller than they were.
Once in the ambulance, breathing oxygen through a mask, I hoped the worst was over. In the E.R, the doctors and nurses asked me, “Can you tell us what’s wrong?”; and, astonished and angry that they couldn’t tell that I couldn't speak, I grabbed the pen from someone’s breast pocket and wrote on the paper sheet on the examining table what had happened and how much epinephrine I had already taken. They changed my oxygen mask for an albuterol one, and within minutes my breathing began to clear — a strange sensation, like someone removing thick cobwebs one by one— and I began to notice my headache and nausea. “That’ll be from the epinephrine,” the nurse said, though she had no idea why, if I had so much of the drug in my system, the attack had ridden roughshod over it. She brought me a bowl, into which I threw up, and acetaminophen suppositories, which I accepted with the lack of dignity of one to whom other people barely exist.
I sat on the table for an hour and a half, unwinding, my muscles unwrapping themselves until I was no longer a clenched triangle but could sit back against the pillow as the external world returned. I felt as if I had been inside out. The staff was as surprised that a major attack had passed so quickly as they were baffled about what had caused it. Within two hours I was shaky but breathing normally; at 4:00 a.m. I shuffled out to the lobby in lime-green hospital Styrofoam slippers and took a taxi home.
In the emergency room, as the attack eased away, I wondered if afterward I would have that transformative experience of seeing the world afresh and anew in all the glory that I had been overlooking; then, when that seemed unlikely, I wondered if I would emerge like Coleridge’s wedding guest, a sadder but a wiser man. In fact, I was no wiser at all, as far as I could tell. Instead, it felt as if I had been visited during the night by a bear that filled the room with a blacker darkness for a terrifying long moment and then lumbered out, leaving me wondering how the hell it got in and whether it could return and leaving also a faint but perfectly distinct odor that might be the creature or might be my own smell of panic.
THE SHAPE Of THE LUNGS, you must understand, is significant.
They look like the roots of a tree, perhaps, though far spongier and more delicate. They begin with a single trunk, the trachea or windpipe, running down from the back of the throat, pink and purple, glistening with the fine coating of mucus that catches stray particles of dust, soot, etc., and is our airway’s first line of defense. Below the base of the neck the trachea branches into two bronchi, one for each lung, each of them not merely a rubbery tube but a highly sensitive and complex environment, with muscled walls capable of expanding and contracting to allow more or less air to pass through (less if the air is suddenly cold, more as one exercises) and a highly specialized skin surface, or epithelium, patrolled by the myriad complex agents of our immune systems and studded with goblet cells that release more or less mucus as the situation demands. Each bronchus branches again and again into smaller and smaller airways called bronchioles (miles of them packed into less space than a gallon jug) and they continue branching until, at their tiniest and most threadlike ends, they blossom into a cluster of budlike alveoli, where the miracle of gas exchange takes place and oxygen passes into the bloodstream without blood seeping into the airways.
This is also what asthma is like. It may sound like one disease, but in fact it may have two entirely different primary symptoms: a wheeze or a cough. And the closer one examines asthma, the more it subdivides. Many people associate asthma with allergies, but it isn’t clear why we have allergies or how we develop them or why they strike different people at different ages or why one person’s allergic reaction takes place in the nose and is called hay fever (or allergic rhinitis) while another takes place in the skin and is called eczema (or atopic dermatitis, “atopic” simply meaning allergic), whereas others take place in the airways and are called asthma (or, nowadays, reactive airways disease). But many asthmas don’t seem to involve allergens at all, being brought on by such apparently benign conditions as laughter or exercise or cold air.
The new thinking is that asthmatics have some unexplainable chronic inflammation that leaves our airway walls permanently swollen and hypersensitive, ready to cringe inward at the slightest threat, strangling our air supply. But neither of these branching, diving explanations accounts for the asthma attacks apparently started by moments of anxiety, nor the fact that an entirely different mechanism, involving an enzyme called cyclooxygenase, can bring on some of the most vicious attacks of all and mean that a single aspirin or ibuprofen tablet could kill me.
This branching airway design is a metaphor for one other feature of asthma, in fact. When we look around us for the potential dangers, the items in the landscape that might kick off my asthma or yours or your neighbor’s, they might be lurking literally anywhere. Allergies may bring it on, but the allergens themselves are almost infinitely diverse: ragweed, beer, shellfish, dust mites, molds, cockroach scales, red wine, grass pollen, peanuts, cat dander, and literally hundreds of others. Soot and dust particles may trigger an attack, or cigarette smoke or car exhaust. Thousands of substances in the workplace can be equally devastating: carpet-cleaning fluids, mildew, toluene diisocyanate, mites in grains and flours, chemicals with syllables too numerous to count, let alone pronounce. It is as if our whole environment in California in 1996 were peppered with asthma mines waiting to go off, or possibly the other way around, that our immune systems are alert to an increasing number of threats in a world we are constantly molding to fit what we think are our best interests.
The Centers for Disease Control in Atlanta reported that between 1980 and 1987 the U.S. death rate from asthma rose 31 percent and has almost doubled in the last ten years. In 1992 about 5000 Americans died of asthma. Six percent of all hospital visits are a result of asthma, with asthma-related health care costing more than $4 billion a year. At least 12 million Americans, and 5 percent of all people in the world, have asthma. The death rate for asthma is rising everywhere. Nobody knows why.
Children in particular seem to be at risk, especially black children, especially those living in inner cities. Perhaps a million children have asthma, which is the commonest reason for them to miss school and one of the most frequent causes of their hospitalization. Childhood asthma deaths rise by about 6 percent per year. Hospital admissions for childhood asthma almost tripled between 1970 and 1980, while all other childhood diseases remained stable. The bulk of the total hospital-admission increase was among children, with black children admitted four times more often as whites.
The official line is that asthma is an incurable but treatable disease, and the vast majority of asthma sufferers ought to be able to live normal lives. After a long period of free-for-all, there is now a set of official guidelines for diagnosis and treatment; and since the introduction of inhaled steroids a little less than a decade ago there are now good drugs that should have the whole issue under control.
Yet asthma is not going away.
By the most optimistic estimates, it is as common as ever, and most physicians fear that unlike almost every other disease, it may actually be on the increase. As the ’90s progressed, more and more doctors appeared in the newspapers admitting that the wonder drugs had not turned the tide, and every so often another death from asthma hits the local or national news, creating a small but disturbing ripple of alarm.
The more I find out about asthma, the less I think of it as a disease and the more it starts to seem like an index of dysfunction. No matter what avenue we venture down, sooner or later we run into a provocative silence or a flurry of contradictory answers.
We learn how our car works when it breaks down; similarly, the presence of a widespread chronic disease, incurable despite our belief in scientific medicine, often severe despite the fact that we should be able to control it easily, indicates an entire network of cracks in the smooth facade of our understanding — of disease, of agriculture and industry, of the family, of social welfare and public health, of ourselves. If we knew more about asthma, we would know a darn sight more about ourselves and about the world.
WHEN WE THINK Of DISEASE, we think of doctors, and we think of doctors curing our disease. This doesn’t work with asthma, not only because asthma is incurable, but because a very strange and usually hidden dynamic exists between asthmatics, their doctors, and their medications. In short, asthmatics tend not to see doctors and not to take medications.
This apparently baffling behavior is due in part to the fact that some asthma medications don’t work especially well, and some tend to draw attention to the self-conscious asthmatic. It’s also due partly to the fact that the critical medications for controlling a long-term incurable disease are preventive and need to be taken for life, and we are accustomed to thinking of medication as something we take only when we absolutely have to and resent it. Above all, though, asthmatics need a very particular kind of doctor.
Michael Welch of the Allergy and Asthma Medical Group and Research Center on Granite Ridge Drive in Mission Village is widely regarded as one of the premier asthma physicians in the country. In part, his reputation comes from the cutting-edge research he and his colleagues are undertaking. (Most clinical allergists do virtually no research; some don’t even read the research.) His associate Carol Gallet showed me what the Pentagon would call the new delivery systems. The aim is to get away from Freon and fluorocarbon propellants and to make more use of powders than atomized liquids. She showed me a state-of-the-art med dispenser that looked like a diaphragm case. You cock its release mechanism, trigger it, and it dispenses a measured dose, simultaneously recording on a small counter how many doses are left/have been used — a very useful safeguard against the panic of a severe attack and a virtually empty inhaler.
Dr. Welch’s office is also testing the first nebulized, inhaled steroid. Previously this was a blind spot. Small children have to use nebulizers (like small humidifiers in which the medication is dissolved) rather than inhalers because the latter require a coordinated in-breath as the med is released, which is too complicated for them. On the other hand, the inhaled steroids that would be very beneficial to young asthmatics wouldn’t dissolve easily enough to be used in a nebulizer. Welch’s office has the first prototype to solve the problem with new soluble steroids.
They’ve also created what Welch jocularly calls the Cat House, a trailer in which patients can be tested for cat allergy and try out a new form of immunotherapy involving T-cells.
The niftiest gadget, though, is called Airwatch. It looks like a three-tone stopwatch-cum-Sega game. This was especially appealing to a kid who had just come from being intubated but, as with many asthmatics, had no interest in learning more about his condition or monitoring his breathing with a peak-flow meter. He had been emptying a Ventolin inhaler a week — toking on it every half-hour, eight times the recommended rate. Airwatch is a small computer. The kid programs it with his normal peak-flow readings, then pulls out a small mouthpiece into which he blows. The readings tell him how freely he is breathing at the moment. At the end of a week he flips open a small cap at the base of the Airwatch to reveal a phone jack. He plugs in the phone line and his readings for the week are transmitted to Palo Alto, where the service is based, and then faxed to his family doctor. It’s something of an upscale service and not cheap — $163 for the first year for the Airwatch plus the service and $100 a year thereafter. But all asthma meds are expensive. The important thing is that the boy might actually use it.
Yet probably the most important reason why Mike Welch is so highly regarded by his patients has nothing to do with his research or his professional qualifications; it is that almost immediately you, the patient, realize he is going to be there for you, which, for someone with a chronic illness, is as important as any other feature of treatment. An asthmatic, whose illness is not only chronic but can be very frightening, needs someone to bond to, someone who is both skillful and caring. “The active presence of the physician,” writes Eric Cassell in The Nature of Suffering, “is part of the treatment.”
After my major attack in November of ’91, I was referred to a physician who was generally regarded as a top asthma specialist. He gave me a prescription for Vanceril, some dosage instructions orally and in writing, and told me to come back once in a few weeks, again in April or May, at the beginning of the pollen season, and again in a year’s time. I didn’t go back for the next appointment; I went back several months later and then skipped the spring appointment and one-year follow-up.
I didn’t go back because I just didn’t believe he was sincerely interested in my welfare. “If you have another attack as serious as this one,” he instructed me, “you must see me at once”; but as I was enfolding myself gratefully in his concern, he added, “during office hours on the next working day."
To hell with that, I thought.
When six or eight weeks went by and no receptionist called to jog my memory about the next appointment, I knew. He didn’t care. He was a specialist with a full waiting room. At a rough guess, he made five times my annual salary, yet the sign in the front office still demanded payment in full at each visit. Fuck him. When I did return, it was, though I didn’t realize it, to prove him wrong. He had said I was probably suffering permanently reduced lung function, by implication because I hadn’t come to see him sooner. When I went back, not having wheezed for four months, I blew so hard into the peak-flow meter the needle went off the chart. Take that.
He had done his best, but instead of getting me to follow the precise duplicated instructions he had handed me, he had pushed me — to be more accurate, I had retreated — into the shadows of medicine. And virtually every asthmatic I’ve talked to has had a similar experience, often, sadly, with more than one doctor. Sara Sweet, of the group Parents of Children with Asthma, took her daughter Bonnie to see one of her HMO’s allergists, who showed her glossy pictures of dust mites and then asked, “Well? Any other questions?” The pediatrician was no better. “Lousy. Unsupportive.” She now pays out of her own pocket to see Welch, who is not on her HMO’s roster.
The three most important qualities for a doctor, wrote Sir William Osier, the great turn-of-the-century physician, are availability, affability, and ability, in that order, and for chronic disease at least, that is still true.
This may be even more true for the parent of a severely asthmatic child, as he or she is not only helpless in the face of an attack but also in the face of his or her failure as a parent. She has tried everything she can for her child, and he is still in unpredictable and desperate danger. In those dark times, it is vital to have a physician who is caring for the parent as well as the child.
“You want to feel as if you have someone who can rescue you and rescue your child,” explained Lynn Devine, who now sees Dr. Welch with her son Alex. “Some of the best doctors in town don’t get that.” Before she saw Mike Welch she took Alex to a doctor named Nevin Wilson, who has since left the area. Wilson recognized the value of Osier’s doctrine to such a degree that he once saw Alex at 10:00 a.m. on Christmas Day.
Without someone to bond to, we may do almost anything, trying increasingly desperate alternative remedies, visit well-meaning and likable doctors who know relatively little about asthma (all too common, sadly), or convince ourselves that our asthma is not all that bad anyway, pushing ourselves further and further into the shadows of medicine and setting ourselves up for that final desperate dash to the ER.
Our defiant and resentful behavior is officially called “non-compliance.” I talked to two nurses in San Diego who couldn’t understand why people with asthma keep smoking, don’t take their meds, or leave it until the last minute to come to the ER. “Most people are really, really stupid,” said one. “No, I think people are just lazy,” said the other.
This is quite wrong and shows how wide a gap now yawns between the world of medicine and the world that medicine is intended to serve. Asthmatics “fail to comply” not because we are congenitally stupid, lazy, or stubborn, but because severe asthma causes a double rejection of reason. In the throes of suffocation we don’t want a cool medical intervention, we want someone to cling to in abject terror. (Lacking a doctor, I called, “Help me. Help me," to a fireman, who was as helpless as I.)
“Asthma is such a frightening disease,” said one of the few doctors I’ve met who understood the needs of the asthmatic, “that an asthmatic wants someone to bond to” — and as soon as he said “bond,” I vividly imagined the doctor I’ve never had, a knowledgeable friend, present and comforting. I saw myself bent over, gripping his arm, trying to breathe, knowing that he could be trusted and that I could allow myself to be seen in this moment of panic and weakness.
Which is, of course, the second rejection of reason. Once the attack is over — which may, after all, be only a few minutes later — the disease seems to vanish, and we are left feeling not only scared to the core but also very foolish. It’s as if a tidal wave had crashed in through our bedroom window in Kansas, overwhelming us, taking us to the point of drowning, and then withdrawing without a trace, the carpet not muddy, the bedclothes not even damp. How can we not be ashamed of our panic, our moment of weakness? This makes it all the harder to go to see a doctor when we have no symptoms to justify our poaching of his time, only an emotional residue that is all the more uncomfortable for having no cause that we can show.
His cool professional manner rebukes our desire to blurt out, “Doctor, I’m scared”; and his trained reply, “What seems to be the trouble?” reminds us that this is supposed to be an intelligent exchange of medical information. So he dismisses and we beg for something more, or else our pride tells us we’d rather go with the patent medicines and try to suppress the anxiety, though to do so will lead us to be accused of denial. All medicine is driven and distorted by fear, and asthmatics are merely an extreme case because the condition is so common, so frightening, and so quickly over. Or maybe the ideal of cool professional detachment is simply the wrong model.
ONE COMMON REASON asthmatics don’t take their meds as prescribed is that they don’t trust drug companies — a distrust that is often so deep that it sucks in doctors who prescribe and therefore apparently endorse not only the drug companies’ products but also their actions. Physicians are, in fact, in a very tricky position in being beholden to their pharmaceutical cousins while having virtually no control over them. Quite the reverse, in fact; the drug companies are not above trying to mislead doctors — indeed, they must impress their products’ effectiveness and reliability on the doctors who will prescribe them or use them in hospitals.
You’d imagine that in the professional periodicals, at least, drug companies would be kept to the straight and narrow, but a 1992 UCLA study of 109 ads in 10 leading medical journals found that 100 contained “deficiencies in areas for which the FDA has established explicit standards for quality.” Forty percent of the ads reviewed exaggerated a drug’s benefits or downplayed its known hazards; 30 percent cited statistics from “inconclusive, dissimilar, or poorly designed studies”; and 30 percent included misleading graphs or tables. If these are the ads directed at those most likely to spot their errors or liberties with the truth, what chance does that leave the muddled layman who is still at the kindergarten level of trying to spell “relief’?
It leaves us watching television news, but there too the drug companies have exerted their influence. A notorious example was the Billie Bloom videotape, which looked like a locally produced spot in the evening news, which aired on KGTV, Channel 10 in San Diego and in other cities in early 1987. Actually, it was a “video news release” produced by a public relations agency in New York, nominally on behalf of the Asthma and Allergy Foundation of America but paid for by Key Pharmaceuticals, a contributor to the foundation and maker of a drug that got a favorable mention in the tape. Billie Bloom, an 11-year-old asthmatic, reenacted on camera an asthma attack that occurred after she had switched medicines. The thrust of the message was that generic drugs can be less safe than brand names — a message that the FDA considered misleading, but it took no action. In all, the New York Times reported, the tape was aired 31 times by 23 stations and was seen by an estimated 1.3 million people.
ONE OF THE MANY MIRAGES CAUSED BY ASTHMA is the belief that if we look at what helps the condition, we may better understand what causes it. The trouble is that over the centuries sufferers have been lured by a wide variety of so-called cures, and astonishingly, many of them have done at least some good. In a sense, asthma is the perfect advertisement for a holistic approach, because any improvement in what is now called “baseline health” tends to lessen asthma symptoms. Or maybe it’s the other way around: asthma, or at least some asthmas, is an illustration of our general health —as a person, as a society, as a planet.
An Egyptian asthmatic of the 16th century B.C. might have been handed a papyrus prescribing boiled and strained colocynth, onion, goose fat, beer, and decayed flesh. Chinese remedies included dried geckos and tea made from cockroach entrails. In fact, many traditional Chinese acupuncture herbal remedies involve making a small beetle eat the herbs and then eating the beetle. In classical Greece it was thought that sulfur, which induces coughing, would help asthmatics cough up whatever was making them wheeze, so kindly guides led asthmatics up to the crater of Mount Etna to inhale the fumes. American folk treatments have included licorice water, apple water, mullein, gum ammoniac, vitamins, cider vinegar, marijuana, and cocaine. Asthmatics have been sent to clinics at the tops of mountains and in the depths of salt mines.
I myself have had desensitizing injections, preventive medications, steroid shots, psychotherapy, and even a course of injections of tobacco leaf, silver, and blackthorn prescribed by a homeopath and gingerly administered by my girlfriend, who was understandably reluctant to jab me in the back of my neck.
Perhaps as many as 80 percent of asthma sufferers have tried a non-mainstream treatment at some time. Our faith in alternative medicine echoes the creed of an earlier doctor. Sir Arthur Conan Doyle: when you have eliminated the impossible, whatever remains, however improbable, is the truth. If Western medicine says asthma is incurable, we’re straight off into the realms of the improbable, sniffing along the trail laid by none other than Sherlock Holmes. This is a logical fallacy, of course — just because orthodox Western medicine has no cure, it doesn’t mean that anyone else does either. But if the local MD can’t do it, then it takes no more than optimism to ferry us into the colorful land of the unlicensed and the unproved; and the hooting derision of the crowd in the white lab coats standing on the shore behind us makes us only more determined to prove them wrong.
In San Diego, I decided to investigate three that were still relatively unfamiliar to me: hypnotherapy, yoga, and acupuncture.
JUST WHEN TOU THOUGHT ASTHMA WAS SIMPLY a matter of allergens and inflammation and could safely be left in the hands of the allergists and immunologists who understand antibodies and chemotactic mediators, Dr. George Pratt of Scripps Memorial Hospital and UCSD includes in his book A Clinical Hypnosis Primer the statement, “By current estimates, 50 to 80 percent of all illness is psychosomatic rather than organic.” This does not mean they are self-inflicted or “all in the mind.” It means that “strong emotional states or unconscious psychological conflicts can in time cause organic symptoms or exacerbate existing organic pathology.” In short, he says, stress can produce just about any physical symptom we can imagine.
Exactly how hypnosis works is something of a mystery, he concedes. The American Society of Clinical Hypnosis has written, “None of the definitions of hypnosis satisfies the criteria for a good scientific theory.” (When I read that I cackled with glee and rubbed my hands together. Exactly the same is true of asthma.) All the same, in 22 years of using hypnosis as a psychotherapeutic tool, he has found it frequently very helpful in treating people to relax, to feel in control, to reduce the frequency and severity of attacks, perhaps by reducing anticipatory anxiety and the fight-or-flight response that sets off the immunological cascade that feels like panic.
His most successful patient, though, was himself. In the early ’80s, at a time of enormous personal stress, he developed adult-onset asthma serious enough to leave him unable to run or take part in sports and to require daily Prednisone and a variety of other meds. After some time he realized he might try some of his own techniques for his own benefit.
“I was so panicked over this I hadn’t thought of doing what theoretically I knew I could do.” He set aside half an hour twice a day to practice self-hypnotic techniques, listening to relaxation tapes that he devised for himself, imagining his niascles getting heavy, feeling comfortable, picturing pleasant scenes, his body beginning to heal, breathing better. He also set up a cue to trigger this relaxation and got to the {joint where he only had to take a break from whatever he was doing, relax his neck and shoulders, and touch his thumb and forefinger. Ten years later he is completely free of asthma symptoms; his chief of staff. Dr. Adrian Jaffer, a renowned allergist, can’t believe it.
The success of Pratt’s hypnosis shows the strange inter-knotted cause-and-effect in asthma. For many asthmatics — but not all — one of our most frightening experiences is that of a severe asthma attack. If fear can provoke asthma, then, fear of asthma can provoke asthma. By extension, anything that mimics asthmatic symptoms can potentially have the same effect, though such facsimiles vary widely from person to person. For years I started wheezing as soon as I swam underwater, as if the sensation of pressure on my chest were a threat in itself or a threat of a threat. (I can’t stand clothes that are tight around my neck either.) A friend is sensitive to rooms with low ceilings, as if physical claustrophobia were a reminder of the internal claustrophobia of asthma. Maybe this is why some of us even seem to be sensitive to changes in air pressure.
This is called “one-trial learning,” Pratt explained. “Anything that reminds you in the least triggers a biological-psychological event.”
This is why, he said, panic attacks and anxiety disorders respond so well to hypnosis. “If you can change the message you’re sending yourself while simultaneously relaxing yourself, you can make a harmless process out of going through an event that would normally elicit a tremendous response.”
Who knows how far afield we scan for such danger signs? Being trapped in an elevator has virtually nothing in common with the physical experience of an asthma attack, yet the fact that we asthmatics instinctively talk of our physical experience in terms of claustrophobia, and the claustrophobe talks of feeling as if he can’t breathe suggests that we feel (the very word has both meanings) in both dimensions. In my phone conversations with my ex-wife, I felt trapped, helpless, unable to speak my mind, forced to hold my breath in the hope that the threat would go away. Is it too fanciful to suggest that in doing so I was creating an emotional-physical landscape that was all too reminiscent of asthma, setting off my own alarm system?
A note: Pratt writes that “a hypnotic suggestion is only effective to the extent that it is accepted by the patient.” The proof of a drug, on the other hand, is that it works irrespective of the patient’s will, and we have come to believe that (1) drugs can cure anything, and (2) because they don’t need our help, we don’t need to make any adjustment in our attitudes or behaviors. We have externalized the responsibility for health and cast it in pill form. Yet this leaves us with profoundly ambivalent attitudes to medicine, as the phrase "a bitter pill” reflects. We want the immediate cure, the magic shot, yet we are terrified of the needle. We want the miracle cure but despise the drug company.
Nowhere is this better illustrated than with asthma, where the miracle drugs — the inhaled steroids — arrived at the beginning of the decade with a loud fanfare that became increasingly muted as asthma continued to flourish. The fact is that drugs, too, are largely dependent for their effectiveness on the patient’s acceptance. If we don’t believe in our meds, we simply don’t take them, or don’t take them properly, or often enough. Meds, like a good diet and regular exercise, must be part of our desires and habits if they are to do any good. The future is not pharmacological.
LINDA ROBINSON DEVELOPED ASTHMA during a bout of pneumonia five years ago. Thereafter, whenever she became anxious or upset, especially during family conflicts with her daughter, she found herself wheezing heavily, unable to finish a sentence. She also wheezed whenever she had a cold or respiratory infection or with exercise.
Six months later she started attending yoga and meditation classes at the Vogel Institute in San Diego. “Almost immediately I noticed a difference. I could stop an attack in the middle.” While arguing with her daughter, “I’m fighting for air, and she got really scared, and she’s freaking out, which helps (the asthmaj escalate even more. Right in the middle of it I was able to relax and change my breathing, so I was breathing diaphragmatically and under control, and after a few minutes my breathing was back to normal.” She still uses her inhaler when she gets a cold, but otherwise she has barely wheezed since.
Yoga has generally good press among asthmatics, but I had never given it a real try, because the only time I took a yoga class I got bored. I decide to give the Vogel Institute a call, and one Thursday evening I find myself in an airy, high-ceilinged room under exposed beams, taking a yoga class with Ken Temple.
The institute, he explains, essentially works on stress reduction and breathing techniques. Yoga, meditation, and deep relaxation, then a breathing technique called prana yama, or the superoxygenation breath, to give more control of breathing, less sense of panic. More esoterically, they teach alternate-nostril breathing, “a way to fine-tune the body’s neurological system.” The spine has two energy systems, he said, one of which arrives at each nostril.
“One heats the system up, the other cools it down.” Breathing with alternate nostrils in a specific way, he said, helps balance the two systems. “The breathing goes to the reptilian brain. It really gets into there, deep and old.”
This sounds pretty esoteric, but the basic concept — breathing from the diaphragm — is familiar to Western medicine.
Many respiratory nurses teach children to breathe from the diaphragm, which lessens the strain on the chest, neck, throat, and back and thus gets more air in with less muscle fatigue and less consequent increase in tension. I can remember relaxing out of asthma attacks up until the age of about 21; after that they seemed to take a firmer grip, and only meds would work.
On the mat, I find that the breathing and stretching loosen up mucus I didn’t know was there, relax muscles I didn’t know I was clenching. I sniff, clear my throat, settle more deeply into the mat. Old injuries reappear in short, sharp twinges; I had no idea I was still guarding them with such silent vehemence. Find the source of the tension; reassure it; relax through and past it. Gone.
Stretching muscles breaks up knots, allowing blood to bring in oxygen and begin healing, flushes out the lactic acid that burns. It releases memories, too. I am 24 again, hunched over in a locker room after a game of squash, feeling the crawling sensation at the base of my throat, trying to release it, feeling with each exhalation the unnaturally long final tapering-off. Don’t fight to breathe in again too soon. Draw down the diaphragm as if it were the bottom of a balloon, pulling air into the lungs without having to use the chest muscles, because they are the ones in trouble, already cramping and twitching, tense, exhausted, sending small stabbing pains between your shoulder blades. Draw down the diaphragm. Let the breath go, slowly, taking its own time. The last few inches of air take forever, but don’t be afraid. Don’t clench. Don’t worry about the wheeze, almost musical at times like a discord on a tiny electric organ. The last few inches of air take forever.
Relaxation is an acquired skill. We are overtly taught how to be hasty or dutiful, how to fight or to grin and bear it, but not how to focus on a particular muscle and relax it. Which is unfortunate, as relaxing is intimately connected to self-knowledge, discovering the body from inside out and thereby discovering the mind and its unexpected quiet authority. After I developed asthma at the age of 11, my mother taught me a few of these tricks, working down the body, focusing on each muscle group in turn, but I suspect she was unusual in this. If you try to force a muscle to stretch, Ken says, it resists — and I’m thinking muscles are like asthma patients, resistant, noncompliant. Fear is stronger than good intentions.
“Asthma is simply a habit of fear, a pattern that can be discarded,” Temple says after the class. “That’s why there is a real cure for asthma in this program. It takes care of that underlying fear.” Everybody has fear, he adds; different people express it in different ways. The crucial thing is not to accept that crippled posture, that crippled self-image, “knowing that our real identity is not the disease.” (He is one of a number of people who believe that to call oneself an asthmatic or an alcoholic is not an acceptance of responsibility for one’s condition but a dangerous tarnishing of one’s own identity.) "We are not isolated beings but are connected within ourselves, with each other, and with the universe.”
Later, a couple of echoes come back to me. Erhard Vogel’s Expert in Life program sounds very much like the advice that physicians who work with chronic illnesses such as asthma and multiple sclerosis give their patients: become an expert in your condition. The take-charge attitude that Mike Welch advocates reappears here, only writ larger and broader. Take charge not only of your illness but of your life in general. It’s a sign of how disease-focused Western medicine has been that we have swallowed this perspective. How can we take charge of a disease without addressing the rest of our lives? This is one of the central problems of asthma. Monitoring my symptoms with a peak-flow meter is indeed one step toward understanding and taking charge of my condition. But how much good does it do if I am stuck in poverty or addicted to cigarettes, or my parents won’t take my illness seriously, or my husband is an alcoholic, and it’s all I can do to keep myself intact?
I can’t speak for Erhard Vogel’s philosophical and therapeutic approaches, having seen virtually nothing of them, but I can’t see how yoga itself can do anything but good — unless it becomes too soothing and we use it as a way to ignore learning about our disease. (It’s all too easy to take Ken Temple’s “Asthma is simply a habit of fear” at face value, nod, and remain in near-total ignorance about what triggers our illness.) Many practitioners of Western medicine are open-minded enough to recommend yoga as part of an asthma treatment; their fear, and mine too, is that their Eastern counterparts won’t grant them the same respect. Taking charge of chronic illness is very difficult without taking a broader grip on one’s situation in life. But taking charge of one’s life should also involve learning about one’s illness, moving back and forth between Eastern and Western approaches with ease, speaking both languages.
George Pratt and Ken Temple use different techniques toward a similar end. Some may work better for some patients, others for others; the degree of belief, in itself, may affect the degree of commitment, of relaxation, and therefore of response. We’re in gray areas here, impossible to quantify. No wonder allergy, with its precise numbers of IgE antibodies, seems so much more credible, so much safer. Whether alternate-nostril breathing really purifies the anabolic and catabolic motor fibers in the spine (as the Vogel Institute literature promises), I can’t say, being a novice.
I didn’t do it. In general, this stuff is impossible to quantify. How much benefit did I get from it, on a scale of I to 10? How much did the guy next to me get out of it? How quickly did it act? Why didn’t I respond as well to yoga when I first tried it 15 years ago? Can the instructor guarantee that his results are reproducible? Are they more effective than placebo in double-blind crossover trials?
(Yet even in conventional medicine, one patient is said to “respond well” to a drug, while another responds less well; we all have different tolerances and different side effects to differing degrees, and when one starts to include the mysterious power of the placebo effect, this yoga stuff is not so weird after all.)
On my way home, I encounter a couple of nurses from Children’s Hospital. They see a lot of asthma: in-patient, ICU, ER. It’s a terrifying thing, they say — for the patient, for the family, for the caregiver. The staff can administer the meds, but then all they can do is watch. Everyone is tense; the families, too, can hardly breathe. The patients are usually silent, hunched over in the classic tripod position, unless they’re very young. The meds make the two-year-olds ballistic, they say, the heart rate way up. Then they may crash, suddenly, their respirations rate dropping like a rock, and then it’s time to intubate them. But this is a last resort. The tube itself is invasive and can make the airways clamp down still harder. And in any case, the respirator tends to work only one way; the positive pressure forces the oxygen in, but there’s no corresponding pressure to force the carbon dioxide out. Asthmatics die with their lungs full of trapped, stale air. This is what we talk about over pad thai and red curry, this and their plans to get away from their work, to visit Australia for a month, to visit the chateaus of the Loire Valley.
THE AIR Of TAI-MAN WANG'S OFFICE IN CLAIREMONT is thick with the strong, barky smell of a thousand herbs. On his desk, under a hundred or so papers, he finds William Chang’s Catalogue and Reference Guide of “Jen-on ” Chinese Herbs and Formulas and shows me some of its descriptions of various asthmas and the recommended remedies. On his shelves stand a collection of mysterious jars of apothecaria and a remarkable range of books in both English and Chinese, books about herbs, about standard Western medicine, a translation of The Yellow Emperor’s Classic of Internal Medicine, which includes what is thought to be the first recorded description of asthma, and, as if to complete the trilogy of alternative cures. Helping Yourself with Self-Hypnosis. I seem to have come full circle.
Wang grew up and trained in Taiwan and came to the U.S. in 1970. He diagnoses by looking at the tongue, reading six pulses on each wrist, palpating key points, testing sensitivity to heat and conductivity. He thereby arrives at a holistic picture of the patient’s general health, the overall flow of his chi energy (a combination of the nervous system plus the electromagnetic closed-circuit system among the tissues, the wired and the wireless) through the meridians that serve the major organs. The flow of energy is regulated by inserting and manipulating needles to stimulate or suppress it. He begins to treat the most acute conditions, then moves on to restore and maintain a general balance of health, both physiological and psychological. Treatment is with needles in the office, with herbs at home, traditionally in tea form, now available as capsules.
He shows me a needle, then with a swift and unexpected flick of the wrist he inserts it into my arm, on the outer curve of the crook of the elbow. It doesn’t hurt as it goes in — a slight shock, perhaps — but after a moment it seems to expand and take up more space, to affect an area roughly the size of a tennis ball. This region feels slightly uncomfortable, a dull ache with an overtone of annoyance, like something that needs to be taken care of but has been put off as long as possible.
As the interview goes on, I find myself clearing my throat every few minutes and am a little embarrassed, then think, screw it. I’m an asthmatic. I produce more mucus than some people. If he can’t deal with it, then he doesn’t deserve to be a doctor.
Two days later I recall this and realize that I don’t clear my throat like that all the time — in fact, the looseness of the mucus started shortly after Wang inserted the needle in my lung meridian and lasted for perhaps half an hour. Have I, in effect, received the beginnings of an acupuncture treatment without even knowing it? My mind boggles, uneasily.
Meanwhile, he reassures me that he refers emergency cases of asthma to the HR, recognizing the need for extreme measures in extreme cases, and advises asthmatics against eating anything cold, such as ice cream, whose temperature “affects the energetic system and delays the recovery.”
In Western terms, these techniques simply shouldn’t work. Some are untested, some unproved, some based on principles that we claim don’t exist. Which is why I am particularly interested to meet Alex Morales, one of Wang’s patients, and his mother, Martha. Before our meeting, she types a two-and-a-half-page letter explaining her ordeal with Alex’s asthma.
I meet them at Wang’s office. Alex does not look like a sufferer. Now 14, he shakes hands firmly, looks relaxed and fit in sneakers, shorts, polo shirt, with longish dirty-blond surfer hair. He starts on the soccer and football teams at Francis Parker School.
Alex suffered his first attack at nine months, Martha says, reading from her account, when the family was living in Phoenix. “I have been blessed with good health, stamina, and vigor all my life. At that time I could not have imagined how his illness would impact our lives.” Over the next five years Alex took Alupent, Bronkosol, Slo-bid, Prednisone, theophylline, epinephrine, Ventolin, and other drugs. “It has been ten years since he took those drugs, and I still remember their names.” He was twice hospitalized; he suffered from accelerated heartbeat, bronchitis, sinus infections, and pneumonia. “He was sick every month for the first 5 years of his life.... He has gone through seven or eight cycles of antibiotics every year for at least 7 years. At age 14 he has taken more antibiotics than I have in 41 years.”
The worst and most constant symptom, Alex adds, was his blocked nose. “It was like I had two pieces of marble shoved up it. I couldn’t sleep well. Phys ed was a no-no. To keep up with my friends when they were running around the playground was hard also. I had to chew with my mouth open, and some days even to talk was hard.”
In 1986, she goes on, she turned to alternative medicines in an effort to wean Alex from the 15 or 20 pills he was taking each day. Over the next six or seven years, Alex submitted to tea of catnip, conifrey, lobelia extract, castor oil packs on the chest and back, glycothalmine in water, steam treatments, Mother Earth cough syrup, massage, postural cupping, herbs of fenugreek and thyme, and chiropractic care to free up the nerves to the nose.
“The beet juice was the worst,” Alex interjects. “It was horrendous.”
“He submitted to everything I did to him,” Martha replies, “but if he had a choice between beet juice and dying, I think he’d rather die.”
She eliminated all meat, dairy, corn, soy, orange juice, artificial coloring and flavoring, sugar, and salt from his diet, then gradually reintroduced each to determine their effects. An allergist said that he was allergic to olive trees. A CAT scan showed nothing wrong with the structure of his skull.
The Morales family had and still has no health insurance. “I have paid out of my pocket for everything,” Martha says.
In the fall of 1995, the Morales family moved to San Diego. “He is now 13,” Martha reads, “and still does not breathe through his nose. Alex has come to accept it. He says, ‘Mom, that is just how I am.’ I say, ‘No. We are treating symptoms and not solving problems.’ He gets sick again. It is now October of 1995. My husband saw Dr. Wang’s ad in the newspaper. I call Dr. Wang. It is 11:30 at night. He answers the phone. Says to bring him in tomorrow at noon. We go. [Dr. Wang) is wonderful. We go 12 times or so, and Alex finally breathes through his nose, slowly at first but then more openly. Dr. Wang has to send to China to get a very specialized medicine to help him.”
On New Year’s Eve, Martha reads, she toasted her son, saying that this would be the first year of wellness in his entire life. “Alex no longer takes any medication at all, thanks to Dr. Wang. God bless Dr. Wang,” she finishes and bursts into tears.
Alex explains that his first impression of acupuncture was not the weirdness of the treatment but the kindness of the doctor, the care with which Wang explained his treatments, the fact that he was going to treat the problem rather than the symptoms.
“It doesn’t hurt,” Alex stresses. He lies down on something like a massage table, Wang positions the needles, sets an electromagnetic lamp over the table to warm the needles, and Alex relaxes. The whole treatment takes an hour to 90 minutes.
He now sees Wang every three weeks. He hasn’t had an infection in four months — a record for him — and he hasn’t used his bronchodilator in two months. New Year’s Eve, a time when he was usually battling bronchitis, he went ballroom dancing at the Marriott Marina with his mother and stepfather.
“You know how some men have a worn patch on the back pocket of their jeans where they always carry their wallet?” Martha asks. “Alex had a worn patch shaped like his inhaler.” Now she looks at his jeans, she says, “and there’s no worn patch. Are they really Alex’s?” She starts crying again.
“If he wanted to marry a girl who had asthma. I’d tell him, ‘Think of her asthma as being like schizophrenia. Now do you want to marry her?’ It changes your life. It changes your whole life.”
A recent issue of the newsletter “Asthma Update” passes on the experience of a doctor from Louisiana who used to treat various pain problems with steroid injections in the upper back (to be precise, in the infraspinatus muscles of the infrascapular fossae). He was surprised to hear that those he had treated who had previously suffered from asthma showed sudden and complete remission. Intrigued, he began examining this area in his asthma patients and discovered that almost all of them found it painful. Was it possible that he had stumbled across an acupuncture point and the injection had in effect acted as an acupuncture needle treatment? Sure enough, there are lung acupuncture points in the vicinity.
In a letter to the journal of Family Practice, the physician reports that he offered steroid shots in the upper back to all his asthma patients and “their asthma was put into instant remission. They no longer wheezed or required ongoing medication and inhalers to breathe. Were they cured? Well, if you use the same standard as for cancer cure (five years without a recurrence), then yes, you must conclude that these asthmatics were cured of asthma.”
If I had a hot dinner for every miracle cure that patients and physicians had told me about, I would be a chubby man. (Blue-green algae was probably the weirdest.) All the same....
OVER THE WEEKEND I TRAVEL DP TO THE MOJAVE DESERT, north of Los Angeles, with the UCSD Cricket Club. This is a paradox, of course. Cricket is played on a grass field, so what are we doing in the land of B-2 bomber bases, bare red mountains, and Joshua trees? The answer, of course, is irrigation, to which the whole city of Victorville, home of the High Desert Cricket Club, is a tribute. We play in the residential development beyond the golf course, next to the artificial lake.
Desert is hypoallergenic: virtually no pollen or mold spores. The clean, warm, dry air is one reason people move here from the damp Northwest and the chilly Northeast. Irrigation — an entire lake, for Pete’s sake — introduces water vapor, which takes whatever airborne allergens are around and holds them in suspension, an aerosol, just like the nebulizers that asthmatics use, perfect for inhalation. Water permits the spread of suburbia, with its lawns and shade trees, and the result is pollen counts and allergic activity utterly abnormal to the region. A number of former desert communities have passed legislation limiting the height to which Bermuda grass may be grown in an effort to limit its seeding and pollination and have even banned mulberry trees, but these are Band-Aid measures.
Irrigation also permits farming, a major source of asthma problems caused by pesticide spraying, but also by more natural causes. “There’s a lot of mold growth that you don’t get in a real desert but you do get in an irrigated desert,” explains Dr. James Ellis, who has been seeing most.of the pediatric allergy cases in the Imperial Valley for 30 years. He sees a lot of children with mold allergy, and the year-round growing season allows no relief from pollen. “My roses — I’m having a heck of a time cutting them back because they won’t stop blooming,*’ he says. Perhaps because of the mild climate, the RSV virus, an especially nasty respiratory virus, also flourishes all year round, irritating airways and triggering asthma.
El Centro has other problems, too, adding up to the characteristic asthma fingerprint distinct to each region. With a prevailing west wind and the city lying in a bowl, below sea level and at the foot of the mountains, El Centro suffers common temperature inversions. When farmers bum field stubble, the smoke often rises about a hundred feet and then moves sideways. This traps smog and pollens that might otherwise disperse. Moreover, winds often blow down from the mountains, bringing pollen from a variety of trees and vegetation higher up. A lot of children are allergic to trees not actually found in El Centro.
Then again, El Centro shares the valley with Mexicali, perhaps ten miles away, where the pollution levels are considerably higher, thanks to emission standards that are more lax than California’s.
After the cricket match in Victorville, played in the brilliant light and limitless visibility of the high desert, we head back in the mid-afternoon. As we wind down the blighted lunar valley toward San Bernardino, the sun is already setting over Los Angeles in a swirl of livid red-purple smog, dwindling long before it reaches the horizon. By 4 p.m., the mountains a mile away on each side of the road are virtually invisible in the filthy air. Heading down into the approaches to the city seems like going underwater, the skinny palms and billboards of the drowned city sticking up motionless into the gloom. The only time I have seen air like this was in photographs of the towns surrounding Mount St. Helens immediately after the eruption.
In the van, my nose begins to itch violently even with the windows closed and only a skylight open a crack. Those of us with slightly tuned-up immune systems, with asthma or allergic rhinitis (alias hay fever) are canaries in the mineshaft of human progress. Any human intervention in the natural world can affect the atmosphere, which is both our most volatile and our most vital medium. The sensitive tissues that come into contact with the air — the delicate linings of our lungs and nasal passages — are constantly presenting us with environmental impact statements we didn’t think to require beforehand.
THE FUTURE FOR ASTHMATICS LIES IN EDUCATION, that subject with which Americans have such a love-hate relationship. A number of doctors have admitted to me that the profession in general does a worse job of teaching parents about asthma than about any other chronic and severe childhood illness. Look at diabetes, for example. If a child is diagnosed as diabetic, the entire family goes straight to the hospital and doesn’t leave until (in theory, at least) they know what the disease is, how to administer the insulin, and what will happen if they don’t.
Many asthma specialists would like to see such aggressive treatment for even mild asthma: but asthma, which is far more common than diabetes, presents a trickier exercise in education. Instead of one shot a day, the child may need three or four doses that, if a nebulizer is needed, require a parent to sit with child in lap for up to a quarter of an hour. Instead of one medication, the pediatrician may have to prescribe two or three, and the sheer process of discovering which medication works best may take six or nine months, during which time the parents become convinced that the doctor is either incompetent or using little Joey as a guinea pig for shady pharmacological experiments. Meanwhile, the asthma may go underground for days, weeks, or even months, making it hard to decide if a course of treatment is working or — this will occur to parents — is even necessary.
Diabetes is simpler. Administer the insulin or your child will go into a coma and may die. Nobody knows when or if disaster will strike an asthmatic; yet even if everything seems okay, the same vigilance must be maintained, the same preventive meds taken. It’s hard to educate under these circumstances, this lack of clear and present danger, and of course the health insurance companies demonstrate their usual don’t-look-at-us attitude by refusing to reimburse physicians or patients for time spent on prevention.
“You see the physician for maybe ten minutes if you’re lucky,” said Mary Beth Parr, currently in charge of asthma education for the Sharp Center for Health Promotion. “They schedule 15-minute blocks for revisits.” When she worked as a nurse in a clinical practice, “I always wanted to take more time with the patients and get to know them on a more personal level, but I was told, ‘Come on, you’re taking too long. I only want you to take vital signs.’ ”
The office was well aware that physicians are not reimbursed for the extensive counseling that a new asthmatic n£eds. The entire frustrating circumstance challenges our understanding of “treatment,” which by implication is swift, diagnostic, and pharmacological. Fifty years ago, with infectious medicine, that may have been true; treatment now needs to involve the active participation of the patient, which means a much higher degree of self-understanding.
And offering education is no guarantee that people will be educated; in fact, the best way to keep a secret is to yell it out loud at an asthma education session. You’d think, for instance, that those with severely asthmatic children would want to get together to share war stories, get tips, draw sustenance from watching others coping. Yet even though Sara Sweet sends out fliers about Parents of Children with Asthma to 2000 patients, the largest meeting was attended by only 22 people; the average is 10 or fewer. Mary Beth Parr has been running one adult and one children’s group per month for a year and a half and has had to cancel more groups than she has run. The largest attendance was 9; perhaps 30 in total have come in 18 months. “Asthmatics think they know everything,” she said. “They don’t see they have a need for additional education.”
The place it is easiest to sell education is in schools; which is just as well, as school populations are rife with asthma. Nationally, 10 million school days are lost each year to asthma. It is the most common cause of missed school days, of children’s visits to the ER, just as it is the number-one cause of hospitalizations for chronic illness and one of the leading causes of work days missed by adults. In 1991 the number of schoolchildren medicated for asthma in San Diego city schools, according to the American Lung Association, was three times higher than those medicated for attention deficit disorder and seven times greater than any other condition.
One in 20 children in San Diego and Imperial Counties, some 47,000 kids, have diagnosed asthma; the total number afflicted is probably double that, because (as in the population at large) those who are least likely to be counted — the poor, the elusive, the immigrant — are most likely to suffer from asthma. Several schools, especially those with a high concentration of military kids, have twice the rate of diagnosed asthma, though this may be a good sign. At least military families have access to health care, and the problem is more likely to be noticed.
Other schools — five in particular, all lying just south of Highway 94 — may have more asthma because the students fit the demographic profile of those at greatest risk. Inner-city blacks and Hispanics everywhere suffer asthma two or three times more severely than whites and Asians.
Schools present a particular series of challenges to asthma care. “Some of the schools are very, very unhealthy environments for asthmatics,” said Janet Wilson, a respiratory therapist at Children’s Hospital, who has aided asthma-education programs in several schools, “and the staff have no instruction in how to improve the situation, and possibly no budget.” Some schools in San Diego don’t even have soap by the sinks, even though hand-washing is a crucial step in preventing the spread of colds and respiratory infections, which in turn are a primary trigger for childhood asthma. Few educators know how important it is to reduce the dust in a school or that industrial cleansing agents may act as asthma triggers.
Moreover, especially in an era of education cuts, schools aren’t set up to give asthmatic children the regular, informed supervision they need. “Getting them treatment on a regular basis is virtually impossible,” said nurse Mary Margaret Loehr, “because in school they’re on a desert island medically.” If a school is used to dealing with medical matters at all, it is used to responding to crisis — the bandage for the cut knee, the quick trip to the ER. But asthma treatment is really about prevention, so every asthmatic child needs a safe and knowledgeable authority figure to look after his medication and make sure he takes it correctly (perhaps 90 percent of children don’t know how to use their inhalers properly) and at regular intervals. Who is that authority figure, if the nurse’s job has been cut to one-third time? When do those medicine breaks take place and where?
Some parents refuse to believe their child is sick and won’t let him or her take an inhaler to school. Some San Diego school districts have no full-time nurse, so the inhaler has to be kept locked up, and the kid has to get someone to open the nurse’s office, which takes precious time and stigmatizes the child. Again, the inertia is against the asthmatic, an outsider, aberrant.
Still, in San Diego it’s not as bad as it is in New York, where in many districts the cuts have eliminated nurses altogether and no meds of any kind may be kept at school. I met a mother who, when her young son had an attack, got a call at the homeless shelter where she lived and had to pick up the inhaler and the baby and walk two or three miles to school.
And yet the most conspicuous signs of hope for improvement are also to be found in the schools, specifically in a program run by the American Lung Association called Open Airways for Schools.
Open Airways grew out of a project developed by Columbia University’s College of Physicians and Surgeons in the late 1980s. “They saw the number of children with asthma coming into the clinic was skyrocketing, and asthma morbidity was increasing,” said Lynn Devine, director of school health programs for ALA of San Diego. The program was designed to reach children at risk who may not normally see a doctor, may not know they have asthma, and may not in fact know anything about asthma at all. The curriculum Columbia developed eventually evolved into posters, handouts, and six 40-minute lessons intended to teach kids that asthma is treatable, that'it does not have to escalate into crisis, that prescribed medications should be taken at the first signs of asthma or cold symptoms, and that children with asthma should live as normally as possible.
When the Columbia team tested Open Airways in New York City among children aged 8 to 11, it found that the children who had completed the program had fewer and less severe asthma episodes but also that their grades improved when they took steps to manage their asthma. Parents reported that they had become more involved, and children without asthma were more willing to help their afflicted peers.
The San Diego Open Airways program started in April ’95 and has rapidly become one of the most successful in the country. “Ninety schools in the first full year of an Open Airways program is remarkable,” said Lynn Devine. Most regions hope for between 10 and 30. The reason, she believes, is that it is run not by a physician but by someone who has learned about asthma through bitter personal experience.
Devine’s second child, a boy, came home from the hospital as a newborn wheezing, although he was six months old before a doctor would diagnose asthma. Now aged six years, he has a variety of severe but maddeningly capricious allergies, has been frequently in hospitals, and has taken a whole basket of meds. A friend once said, “This is like having a disabled child,” but it is possibly more frightening than many more stable disabilities, with its sudden attacks, its dangers lurking in everyday guises — cinnamon toast — the frequent life-or-death rushes to the ER. As a result, Devine has a passionate concern that the school nurse may lack and also knows what can now be done to help even a severely asthmatic child.
In one school she saw a child who was in obvious difficulty. “When the teachers said, ‘Oh, he’s always like that,’ I was able to say, ‘I have a severely asthmatic child at home who has been written up in medical journals because his asthma is so severe. I know what a severe asthmatic is supposed to be like, and if I brought him in you wouldn’t know he was a severe asthmatic.’ ”
Mary Beth Parr is one of many nurses, respiratory therapists, firefighters, and volunteers who took the Open Airways training. Last November she ran a six-week Open Airways course at the Silver Strand Elementary School in Coronado, one 40-minute session a week. The course was offered during regular class hours, at varying times so the same classes would not be repeatedly affected. “We had the best time. It was a blast.” She had 15 kids, mostly in fourth and fifth grade. Some took the materials home. One little girl was in complete denial about her asthma and wouldn’t even take the handout materials home, but most were much more actively involved. Six of the 15 parents attended the graduation ceremony, all said they had learned something.
With children as with adults, the challenge is to change the paradigm, to stop people thinking of medicine as a response to a crisis and to start thinking of prevention. (Time after time I hear asthmatics say that they’ve been on the inhaled steroids — the preventive medication — for a few weeks now, and they’re feeling so much better that they’ve started to cut down on all the drugs they’re taking. The first ones to go, of course, are the preventives, and the whole cycle starts back up again.) It’s very, very hard to convince someone, adult or child, to take a preventive, maintenance medication, Lynn Devine admits. She uses the sunscreen analogy. Mothers put sunscreen on their children before they go to the beach; think of asthma medication as sunscreen for the lungs.
Devine has visited about 40 schools, almost all elementary. There really isn’t a comparable program for junior high and high schools in San Diego. Of the 90 schools taking part in Open Airways this school year, 5 are junior highs, the rest elementary. “At that age they’re young enough to still take it from an adult. At high school they don’t want to hear it anymore,” Devine said. But that’s exactly the problem. At high school age, kids are least likely to behave wisely and in their own interests, even — especially, in some cases — if their lives are at stake. Peer pressure is at its strongest, and nobody wants to look like a geek. Every teenager wants to prove his independence, so who wants to be dependent on meds or be seen to be submissive to Mom’s worried nagging? Not to mention the fact that multiple hits from an albuterol inhaler will give you a buzz....
Open Airways is, in reality, only a start. According to Devine, “The program is finally acknowledging that there is a huge problem. The general attitude among teachers and the public at large is that asthma is as annoying as head lice and not much more dangerous. In the last couple of years 13 kids in L.A. have died from asthma. They don’t realize that even mild asthmatics can have a severe episode and die.”
The death of model Krissy Taylor seems to have been noticed by the high school community, thanks to her frequent appearances in Seventeen magazine. What may or may not have been picked up by teenagers is that she was using Primatene, an over-the-counter inhaler that is not recommended by doctors, or that asthma inhalers, which can give a buzz not unlike cigarettes, are the medication most frequently abused by dieters, after laxatives. People, in putting the unfortunate Taylor on their cover after her death, may have had as much effect as a hundred Open Airways programs. Or not. We’ll never know.
ANOTHER OPPORTUNITY FOR EDUCATION is the annual asthma camp, called Scamp Camp, after the Southern California Asthma Medical Program. This weeklong American Lung Association camp is held annually at Camp Marston, a YMCA camp at Julian, for roughly a hundred kids aged 8 to 13. Four daily medication sessions before meals and before bedtime are used to make medication normal, habitual. The kids also spend a little time learning about asthma. One of the most popular activities is the pigs’ lungs demonstration. Mike Welch brings in a compressor and pigs’ lungs so the children can start to visualize what is going on inside them, inflating and deflating the lungs, explaining lobes, bronchi, trachea. “They think it’s wonderful,” said Janet Wilson, who has volunteered at Scamp Camp. “It’s very gross, and kids just love gross stuff.”
The aim is also simply to provide a camp for kids with asthma. In many cases, these are kids who have never been allowed to go to camp for fear they would have an attack or receive inadequate supervision or simply not be able to take part in many of the activities. Some of the parents, then, see the asthma camp as a chance for their children to learn about asthma; for other parents it’s simply a chance to get the kids out of the house — a common enough motive for camp, but one that in this case might have the extra dimension of respite for the family. Having a severely asthmatic child is very demanding on the entire family. “For some of (the parents},” Wilson said, unaware of the loaded phrase she was using, “it’s the first breath of fresh air they’ve had.” The asthma metaphor works on both sides. In a sense, the entire family is suffocating.
ASTHMA DEMANDS A RADICAL CHANGE DI THE WAY SCHOOLS care for their kids. For example, asthma is all too often a furtive, almost invisible disease. The most dangerous situation is the kid who is using his inhaler every 20 minutes, wiring his metabolism from the medication but doing less and less good. Who sees this? If the kid is moving from room to room and class to class and doesn’t report his condition to the nurse, who knows? And this is exactly the profile for the worst-case outcome, the chronic but manageable condition creeping through the gray into the red zone without anyone around realizing how bad this could get. Then the collapse, the dash to the ER.
How do you monitor such a child? How do you make sure that good, regular prevention takes place, that he takes his meds as and when he should? Lynn Devine’s prescription: kids with moderate to severe asthma should have their medications in the classroom with them, but held by a teacher so that someone in a responsible position knows if the situation is starting to look dicey. (“Teachers will hate this,” she said, knowing full well how the coach is going to feel about having to sign in and carry eight inhalers in his bag to remember to give back at the end of class while everyone is off to the showers.) And those with severe asthma? Well, all severe asthmatics are recommended to carry a syringe full of epinephrine with them at all times. I can just imagine the principal’s face. A syringe?
What she is asking for involves a political change of the hardest sort. She wants the child to have the power to be able to say to an adult, “When I say I’m not feeling good, you have to listen to me.” By all accounts, this is especially hard where that power relationship is most overt — that is, in phys ed, especially in junior high schools and high schools. The coaches are seen as the dinosaurs here, the last perpetrators of the suck-it-up attitude. It’s not that the coach doesn’t understand asthma, it’s that he is more used to believing in authority. After all, isn’t physical education about the perfecting of the body so we don’t have to worry about it, he thinks, remembering the good old days when he could just tell them, “No pain, no gain,” or “Just do it,” and they’d blink and swallow and say, “Okay, Coach”? And thank him in the end, dammit.
Open Airways is good news, and I wish Devine and her colleagues every success. But the fact that things are going well in elementary schools shows our weaknesses and failings elsewhere. First, I tend to agree with Devine when she attributes her success to the fact that she isn’t a physician or a nurse but is driven by the passion and urgency of someone who has had a severely asthmatic child. She is, perhaps, not an expert in asthma but an expert in asthmatics. It is very rare to come across someone with medical training who recognizes how serious and frightening asthma is. When they call it a disease of neglect, they tend to overlook their own role in that neglect.
Second, the Open Airways program reflects the bizarre American attitude that we can and should care for children in precisely the areas that we cannot and should not care for adults. (The current V-chip television debate shows the same odd beliefs — that we have no right to control the content of television in the name of the general public, but we have every right and obligation to do so in the name of our children.) Asthma is just one of the diseases that flourishes in the absence of any semblance of a coherent and thoughtful social welfare system. Sickness is one of America’s punishments for being poor. Children, however, are seen as deserving better; but even so, it is worth noting that Open Airways is carried out voluntarily and by a nonprofit agency. Despite the Airwatch and advances in soluble inhaled steroids, America’s general care for Americans is still locked in the 19th Century.
Third, it’s also significant that Open Airways is being carried out in the schools. One result of this strange contrast between libertarianism for adults and protectionism for children is that schools are and will continue to be increasingly laden with the burden of fixing the ills (and illnesses) of society at large. (Hence the paradox of my daughter being taught in third grade that pollution is wrong on the same day the states were allowed to raise or even abolish speed limits.) And the younger the children, the more this is and will continue to be true. Open Airways doesn’t even try to address the issues at high school, where things are in some respects most difficult.
No matter how well-designed and well-delivered the program's message is, it comes down to 11-year-olds being given one message for six weeks. Who will carry on that torch? Who will maintain the consistency of that message in the face of Joe Charnel and a thousand other dangerous seductions?
IN SCKIPPS CLINIC, WHERE SOME GROUNDBREAKING RESEARCH into asthma and allergies has been taking place, I find myself sitting in on a lunchtime presentation by a drug company rep. His company has collaborated with the National Jewish Center for Immunology and Respiratory Medicine in Denver, arguably the top asthma center in the country, to produce a series of asthma education presentations, complete with four-color transparencies and slick handouts. While a dozen or so doctors and nurses eat gourmet pizza, he runs through his rap to solicit constructive criticism, partly because he wants to make sure his materials are accurate and useful, partly because he is hoping that Scripps will sign off on his project, allowing him access to the clinic’s patients.
The presentation is familiar stuff, pitched to an educated, middle-class, suburban audience, delivered in a jokey style. The Scripps people interrupt with corrections and questions. At one point the rep says, "Above all, I want to make Scripps Clinic happy.” Surely you mean Scripps Clinic’s patients, someone interjected. Of course, he said. Of course.
Did anyone see any ethical problem with a drug company employee making a direct representation to the public? “No,” three or four voices said immediately. Scripps had made sure that the drug company’s name would not appear on any of the presentation materials. Besides which, the rep added heatedly, promoting his own wares would be not only unethical but stupid. If there was one thing he didn’t want to do, he said, it was to get Scripps Clinic mad at him. “Several of my best clients are in this room.”
This cuts both ways. By erasing this professional affiliation, he is less clearly promoting his particular employer, but by the same token he is in effect, if not in name, presenting himself less as a drug company rep and more as a health educator, even a member of the medical profession.
In a sense, these objections are moot. Unless he knows something that Mary Beth Parr and Lynn Devine don't, he simply won’t have an audience, and the ethical question of drug companies pitching straight to the public won’t matter. I just think it’s interesting that, by all accounts, doctors can’t afford the time or the money to spend an hour or more with each patient, carrying out the education that may make the difference between gradual improvement and gradual decline; and insurance companies can’t afford to reimburse time spent on patient education, yet drug companies have enough free cash to research and develop their own education materials and pay someone to take them to the public.
THE BLEAKEST VANTAGE POINT FROM WHICH TO WATCH asthma — and to see all the cracks in what we flatteringly call a health-care system — is from the place where all the asthma failures end up: the emergency room.
Mary Margaret Loehr is a nurse in the emergency department at Scripps Memorial Hospital, Chula Vista. I had always assumed that once someone suffering from a life-threatening asthma attack reached the ER, the danger was more or less over. Wrong. She starts with inhaled beta-agonists, usually administered through a mask. In many cases the problem is the advanced inflammation, the airways swollen until they’re almost blocked, rampant with eosinophils and flaming with an internal biochemical warfare. This needs heavy doses of corticosteroids, either orally or through an IV, hut they won’t do much good for several hours.
If things look grim, she’ll administer a shot of epinephrine (adrenaline) or its cousin, terbutaline, which doesn’t have epi’s cardiac side effects. Some have to have the injection even if they have heart disease because otherwise they’ll die. The last resort is intubation — that is, literally sticking a tube down the throat into the lungs. This is such a traumatic procedure for someone who already can’t breathe that she’ll often have to paralyze and anaesthetize the patient.
“It’s a step to be taken with great trepidation. When you put them on a ventilator, your problems are just beginning. A severe asthmatic is very vulnerable to the increased pressure of the air being forced in and can easily blow out a lung.”
The classic asthma death is one with a slowly dawning sense of disaster. In fact, one of the common features is that the patient has no idea how compromised her breathing is, how bad things are getting. Typically, she is having some trouble breathing — nothing unusual there — and takes the inhaler every four hours, then every two as the relief gets shallower and shorter, then finally every 15 minutes. At some point, she realizes the inhaler is doing no good anymore and is having an increasingly toxic effect on her system. Her head is buzzing, she can’t think clearly. By the time she gets to the E.R, she has large clumps of thick mucus that can’t be dissolved, her airways are so swollen they' are clamped shut, and she dies.
Loehr is disturbed by a series of recent deaths that don’t fit this profile. What she and the paramedics have been seeing more often is a different scenario, one that should be extremely rare. At noon a young woman is walking with friends, apparently well; she says, “I don’t feel so good. I’d better use my inhaler.” Within minutes this becomes, “You’d better call 911,” and she is at death’s door with a terrifying suddenness. Whether this is just a statistical blip or not it’s hard to say, but combining her own experience with those of the local paramedics, Loehr said, “We’ve had a number of stories that were very clear cut. We’ve had several of those just in our own hospital.”
She suspects that familiarity has bred a dangerous contempt, or at least complacency — or maybe it’s the beta-agonist inhaler that has done so, making people think that asthma is trivial, that a single puff will take care of it. And it’s true that the vast majority of asthmatics, like diabetics, can lead normal active lives. But that very normality is deceiving. The paramedics see it all the time, she said. Johnnie takes his Cromolyn, runs with the soccer team, does fine. Coach is happy, Johnnie is happy that this asthma is no big deal, doesn’t keep him off the team, doesn’t make him look like a geek to his girlfriend. Then a time comes when the Cromolyn doesn’t seem to be working, nor do a second and third dose; it never occurs to him that this is a different beast. Asthma is a moving target.
Loehr also sees the patients who never appear in the suburban specialist’s office, whose only point of contact with modern American medicine, in fact, is the dash to the ER. In most cases, these are the very poor; and the very poor are far more likely to suffer from asthma.
The rise in the incidence of severe asthma in the U.S., which can be charted from the late 1970s, accompanies the steadily growing disparity between the increasing wealth of the wealthiest Americans and the increasing number of Americans who find themselves below the federal poverty standard.
Even more striking is the parallel between the rise in asthma among women and the feminization of poverty. Between 1979 and 1988, nearly a million families headed by women fell into poverty, until nearly half of the families headed by women were officially poor, a figure that rises to three-quarters among African Americans. Over the same period, asthma rates among women jumped dramatically. In 1980 slightly more males than females had asthma — 32 as opposed to 30 per thousand, according to the Centers for Disease Control — but by 1990 45 women per thousand had the disease, as opposed to 40 men. Most alarmingly, the number of women dying of asthma jumped 54 percent during the 1980s, compared to a 23 percent rise for men.
Asthma is one of the presenting symptoms of poverty. The fact that the wealthy also wheeze tends to cloud the fact that asthma is, in fact, a class issue. Studies in New Zealand, Scotland, and Britain have found that asthma is worst among low-income and one-parent families. At one time, I joined a mobile medical unit to visit a shelter for homeless families in New York. During the day, a couple of dozen families came out to the medical van parked outside the shelter, and whatever the reason for their wanting treatment, we found asthma in every single family.
The asthma itself has a further economic impact, contributing to a downward spiral. A New Zealand study of 93 adults attending a hospital-based clinic serving “a socially disadvantaged urban population” found that “repeated hospital admissions and frequent asthma-related sick days contributed to employer discrimination, job dismissal, and lack of career advancement.” Thirty-two percent of those currently employed said that they had difficulty getting time off work to attend the asthma clinic. Of those not working, 8.3 percent had lost their jobs because of asthma.
In the U.S., of course, poverty is intimately associated with race, and the black-white gap, always wide, has been widening. In 1979, blacks were about twice as likely as whites to die of asthma; by 1987 they were three times as likely, with the rate among black women ris-ing twice as fast as that among whites. In 1987, asthma death rates in East Harlem were nearly ten times the national average.
Physicians have been aware of the possible connections between these figures, but doctors are not known for being politically radical, and most researchers spend as little time as possible studying the poor. The experts tend to be quoted as saying that “the mechanisms involved” — that is, why the poor should get asthma — “are not well understood.”
Asthma is only one of the many burdens of poverty, its wheeze almost a metaphor for someone struggling to get along with the weight of the world on her shoulders. Under these circumstances, it seems almost a condition of existence, and as such it’s hardly surprising that it is hardly noticed, let alone treated. What can you expect? Why hope for more?
This hopeless and desperate outlook is the breeding ground for all kinds of pathologies, not just asthma. Many of those Loehr sees, especially those she sees regularly, are people who don’t appreciate the need for regular health care and immunizations, or who recognize the need but simply have no means of getting to a doctor, or who have no money and don t realize that some clinics may offer free care, or are too proud, or who simply have a very disorganized approach to life so that making and keeping an appointment is too much for them to handle.
A patient came in who was drunk and had lost her inhaler. Rather than giving her a prescription, which would have been beyond her ability to get filled, Loehr gave her an inhaler. A day or two later she was back again, drunk again, having lost that inhaler too. “There’s no way to link that asthmatic up to routine care, which is what she needs.”
For someone like this (and, arguably, for everyone), the need is for home care. America’s near-complete lack of home care is partly the result of a public failure of commitment; but, Loehr pointed out, countries such as Norway and the UK, which offer medical care that includes routine home visits, have no ghettos, no gang warfare, fewer homeless, few areas where it is unsafe for a nurse to walk in the daytime. (Of course, this raises the question of whether the lack of home health care is the result or the partial cause of these problems.)
And what if a health-care worker could make a home visit and meet a family with five children, all of whom were inadequately clothed, sheltered, immunized, and nourished, as well as suffering from asthma? Where should the medical dollar go? And if, as may well be the case, the problem is compounded by the parents’ pathologies, the visiting nurse is stymied, Loehr explained. The U.S. also has no social mechanism for removing kids from parents who are drug or alcohol addicted. The child’s asthma becomes a symptom, an index of the dysfunction of both the family and of America’s puny attempts at social welfare.
IT IS COMMON — IT'S ALMOST A RULE, IN FACT — to end articles about medicine in one of two ways. Either the last paragraph or two speaks of new research being conducted in a university somewhere and holds out hope of a cure, or the entire tenor of the piece is alarmist, and we are left with the fear that the latest virus or re-emergent bacterium has only to catch a plane to reach us, and humankind is only a breath away from epidemic extinction.
Dr. Edward Golub, formerly a professor of biology and director of research in the pharmaceutical industry, is now president of the Pacific Center for Ethics and Applied Biology and a partner in a group currently developing an interactive program for medical education that may be offered through an on-line virtual university. Dr. Golub suggests a different way of looking at asthma and at medicine in general.
In fact, suggests Dr. Golub, who lives in Solana Beach, most of us have always been wrong about how scientific medicine works. The Salk paradigm, the one-pathogen, one-illness, one-set-of-symptoms, one-treatment, one-drug, one-cure, one-happy-family view, the linear understanding of medicine that he constantly refers to as “the magic-bullet view,” doesn’t work with asthma, and in fact doesn’t work for most illnesses. Medicine never was this simple, although the history of medicine is often told as if it were. The decisive advances were always more subtle, broader-reaching than one drug: the introduction of sewers, the fluoridation of public water. These advances were not good stories and made no heroes. They were unglamorous and rarely the work of a single noble-browed (or Nobel-browed) genius.
The general future of disease will not be the single epidemic horror-virus such as Ebola; it will be endemic rather than epidemic, complex and nonlinear rather than singular. Asthma is a perfect candidate for disease of the future, as are panic attacks, depression, migraine, cancer, AIDS, MS, and the other autoimmune diseases. All of them flourish not in bad drains or mosquito swamps but in the weedy cracks in our paradigms for disease and health, in the dark spaces in our means of delivering health care.
He expands on ideas that he has set out in his book The Limits of Medicine. “The paradigm we’ve been functioning under since, say, 1920 is that health is the absence of disease, and it’s achieved through magic bullets provided by the biomedical-industrial complex, that because we are scientists and physicians and caring people, we’ve taken on almost a civic duty of taking care of the health of the nation. Everybody believed that, and they believed that (a) because we bedazzled them with science and (b) because nobody paid for the product, there were always third-party payers.”
Our faith in the ability of scientific medicine — that is, the biomedical-industrial complex — to find cures for all diseases was bolstered by the fact that from roughly 1945 onwards, newspapers and magazines told us repeatedly that our understanding of this or that disease was advancing and a cure was just around the corner. Our doctors’ powers over life, death, and even non-medical social problems were meanwhile being trumpeted on the new medium of television. More than a hundred American TV series featured doctors as heroes, far more than any other profession. The hospital became the place to rush in search of a cure, and instead of being a humble profession, medicine became a heroic one — not to mention a far more lucrative one.
Between 1950 and 1970, doctors’salaries nearly quadrupled, rising at almost twice the rate of college teachers’. (Drug companies have also been one of the most consistently profitable sectors of the American economy.) The country doctor described by Chekhov and William Carlos Williams still existed, but in popular culture his place had been rudely usurped by Dr. Kildare, and the doctor was replacing the cowboy as the mythic hero in whom a public, bewildered and impressed by the magical advances in medical science, could place its trust.
“Because it was such an appealing and free way of looking at things,” Golub went on, “and because during the era of infectious diseases it really worked, the public overlooked the fact that it was, in fact, a very, very, very lucrative operation, that the complex made scads of money, scads of prestige. Now things are changing. The very success of the system has caused the nature of disease to change. With the introduction of antibiotics, with public health and increases in the standard of living, by 1945 infectious diseases were so far in decline that they were manageable. With that came a steady decrease in infant mortality and a consequent lengthening of the life span.
“As [infectious] disease changed to chronic disease, there are no more cures. We can ameliorate symptoms, but we don’t talk about ameliorating symptoms. We still talk about curing disease. If you look at the fundraising from any one of the disease groups, it always ends. The cure is not here yet....’ It would be unthinkable to go around raising money by saying, ‘There will be no cure, but we might be able to find ways of preventing symptoms.’”
The perfect illustration of that, I suggested, is the for-profit cancer hospitals, which depict individual success stories of people who are still alive five years later. That is presented as a cure, even though that specific word may not be used.
“You don’t even have to go there. You can go to a not-for-profit major medical center. You show up there with a brain tumor. You’ll be told, ‘We’ll take care of everything. We’ll make arrangements for you to meet the radiologist who’s going to zap you, with the oncologist who’s going to treat you with these very, very toxic drugs, with the surgeon who’s going to go in and take out as much...and listen, I saw a patient with a tumor that size who recovered.’ Now the fact is that a young doctor probably has not seen such a patient but has heard from other doctors that every once in a while somebody does [survive]. But these people have never bothered to think about actual outcomes. It’s part of their training, it’s part of the ethos that this is what we do; and what’s expected when you die is that your survivors give comfort to the doctor for losing. So there’s nobody who is innocent here. Patients want to hear it.
“We are seeing, now, the beginning of a paradigm shift. The public confidence that the complex used to be able to count on has eroded. The flip side of gullibility is distrust and litigiousness. It’s no accident that now more office visits are made to practitioners of alternative medicine than scientific medicine. Far more out-of-pocket money is spent on alternative medicine than on standard medicine. The same people, by and large, go to their standard doctor, their insurance company pays for it, they’re not satisfied, and they try aromatherapy.”
This is particularly true, I suggested, of a chronic disease like asthma.
“Sure. Science itself is showing us how complex chronic diseases are, and it will be a miracle if we find actual cures for any of them. The Human Genome Project is just a logical extension of looking for specific magic bullets. The public is slowly and now more rapidly becoming dissatisfied, and the paradigm shift that is already becoming evident is redefining health, not as the absence of disease but as the presence of wellness. It’s starting with the educated higher-income population. I don’t know how far down it will trickle, but it’s no accident that smoking is falling off among educated people. It’s no accident that there has been a 25 percent decrease in cardiovascular disease in the last ten years in the absence of any medical advances, but largely through changes in diet.
“With this change comes a whole new definition of medicine and a whole new role for the doc. The doc is not there to find a magic bullet to cure you. The whole system is going to have to be there to help prevent, to help you change lifestyle, to help augment changes that are made, and to ameliorate symptoms, to delay the onset of debilitating chronic disease.”
The word “doctor” will have to return to its roots. It originally meant “teacher.” The old aggressive metaphors of “fighting” disease need to be quietly phased out, too, given that winning will no longer be an option; perhaps “coaching” might be a better metaphor.
“There was a recent article in Nature/Medicine by some people at MIT. The assumptions behind all the enormous amount of spending, primarily by the NIH, but also by the pharmaceutical companies, is that if we do science we’ll learn two things. We’ll learn how the world works, and because of that we’ll learn how to control the world. That’s what every scientist is taught. What [the authors of the article] point out is that we have been astonishingly successful, beyond our wildest dreams, in the first part. We really know how the biological world works. Not completely, but if you had told me when I started out in graduate school that we’d be cloning and sequencing genes, I would have said you’re nuts.
“And we’ve assumed that if we know how things work, the corollary would also be true, and we’d be able to control things. [The authors] point out that between 1935 and 1946 this really did work. If you look at the number of diseases for which an understanding gave you a treatment, it was astonishing. But if you look from 1946 on, there are few. Very few. And in fact there are new diseases which we can’t deal with. So even with all this enormous increase [in knowledge] the second part is not working, and maybe we have to start rethinking the premise.
“Now, that would be hard enough for the medical-industrial complex to do. It would be virtually impossible for the public. How are you going to tell them cancer is not going to be cured? We may delay it, we may prevent it, but it is not going to be cured. There may be no magic bullet for asthma.”
It’s true. How can one stop the runaway train of our belief in science to find a cure? Perhaps the asthmatic, then, especially the young asthmatic, is at the cutting edge in a change in all our perceptions, a new modesty of expectations. It is often said of childhood asthmatics that they display unusual maturity, a rare understanding of their abilities and their limits. Perhaps there can be nothing better and saner than to have a chronic but manageable disease, whose best and only treatment is to develop self-knowledge — that is, to understand oneself and one’s illness well enough to manage it successfully, to go beyond the frantic chase after illusory cures. Perhaps life itself involves such restrictions and flourishes within such limits.
Why Is Asthma on the Increase?
Some doctors argue that it isn't; it is simpty being better and more frequently diagnosed. The balance of opinion, though, is that more asthma is being diagnosed and more asthma is happening out there, especially severe asthma.
The temptation is to look for one cause, but asthma rejects such simplistic thinking. There are probably dozens of reasons, some overlapping, some nudging each other into action. For example:
Day Care. The number of children in day care has risen dramatically in the last 30 years. Perhaps a third of American three-to four-year-olds attend day care or preschool (in other countries, such as France, the percentage is even higher) where respiratory infections, the most common harbingers of pediatric asthma, run rampant.
Cats. In the last half-century, America’s affections have switched from dogs to cats, and the barnyard mouser has come indoors. Cat allergens (flakes of dead skin and hair) can linger in carpets and furniture for up to 24 weeks after the cat has been removed. Cat dander is such a powerful and easily transmitted allergen that it travels on people's clothes in astonishing quantities. A study in Sweden found higher levels of cat allergen in school classrooms than in some homes with cats, and recent research has even found high levels of cat dander in model homes in which no one has ever lived.
Dust Mites. In a curious way, dust mites suggest a weird link between asthma and comfort. For example, in a group of villages in Papua New Guinea, the incidence of asthma has risen from virtually nothing to more than 7 percent (in other words. Western levels) in the last quarter-century. Researchers discovered that over this period the New Guineans, who once had slept on bare earth floors, had acquired blankets, and the blankets were the first soft materials in these Spartan villages where dust mites could live and breed. Dust mites also flourish thanks to other modem conveniences:
Central heating. Modem climate control indoors ensures that dust mites and some molds can now have a year-round growing season.
Laundry detergents. Fifty years ago. everyone washed clothes and linens in hot water, which killed the thousands of dust mites inhabiting them. Now that we have developed cold-water detergents, the mites remain uncooked and emerge unaffected by water or soap.
Wall-to-wall carpeting. Once the preserve of the rich, it’s now a common feature of tract homes. The more the carpet, the more the mites.
Smoking. The only growth sector in the domestic tobacco market in recent years has been young women in their late teens and early 20s — in other words, in their prime childbearing years. Smoking both during and after pregnancy correlates with a greater likelihood of the child developing allergies, asthma, and respiratory problems of all kinds. But smoking is unlikely to be a growth factor in San Diego, which, according to the American Lung Association, has a lower smoking rate than any other major U.S. city.
Tim Brookes is the author of a book on asthma. Catching My Breath. He teaches at the University of Vermont and is a correspondent for National Public Radio.
Here's something you might be interested in.
Why San Diego asthmatics won't take their meds
Breathless
Why San Diego asthmatics won't take their meds
Breathless
Lynn Devine: “You want to feel as if you have someone who can rescue you."
THIS IS WHAT ONE KIND OF BAD ASTHMA ATTACK IS LIKE.
At half-past midnight on a November night in 1991, my stomach suddenly felt uneasy. This was hardly unusual. For the past month, barely a day had gone by without heartburn. I sat up in bed and groped around for the Rolaids. By the time I found them, my stomach was acidic, turbulent. I ate two. Within a few minutes my entire metabolism changed,
Michael Welch, one of the premier asthma physicians in the country.
My sinuses were swelling, stiffening, filling up, my ears and cheeks were getting hot, my spine and my chin itched. Everything was closing in around my throat and chest; I felt a frightening internal claustrophobia, a sense of metabolic urgency rapidly mounting toward panic.
Edward Vogel demonstrating alternate nostril breathing
I already knew this was no ordinary asthma attack. I had my first attack nearly 30 years before, and over the years I came to recognize several kinds of asthma. Most were a lighter or heavier wheeze that came on gradually, last thing at night, or more suddenly when shoveling snow in a heavy coat. They sounded like the word “asthma,” a sibilant rasp.
The Airwatch readings tell him how freely he is breathing at the moment.
Three times since I’d turned 30, though, something entirely different had happened; a sudden, overwhelming assault had stormed through my whole body, seizing my throat and suffocating me. This felt like one of those asthmas.
Tai-Nan Wang. “Alex no longer takes any medication at all, thanks to Dr. Wang."
I swung my legs over the side of the bed and put my palms on my knees in the classic asthma breathing position, wondering what the hell had brought on this attack. It felt as if I’d eaten something I was allergic to, what with the reaction throughout my whole body, the weird stomach.
Dr. Edward Golub suggests a different way of looking at asthma.
But what had I eaten? Fontina cheese and crackers; a bottle of Dos Equis and a bottle of Grolsch; pumpkin pie and ice cream — nothing I hadn’t had before. Rolaids? I’d been taking them for a decade. They didn’t contain aspirin, did they? Weren’t they just chalk?
Well, what about stress? Christ, what stress wasn’t I under? I was going through a divorce, I was teaching four classes at the university on top of my usual freelance writing— but could stress really cause an attack this bad?
I fumbled around on my night table and found a Primatene inhaler, the kind you see advertised on television with lackie Joyner-Kersee taking a quick hit, recovering in 15 seconds, and then sprinting to a gold medal. It’s an over-the-counter medication the doctors view askance, knowing its predilection for unfortunate cardiac side effects: raised blood pressure, even heart attacks. But my prescribed albuterol inhaler didn't seem to help much anymore; I suspected I was becoming allergic to the propellant — a disturbing thought. The Primatene seemed to work better, so my GP shrugged and said, “Sure. Give it a try.’’ I squeezed the Primatene and drew the spray in deeply.
For a few seconds I thought it had worked. But even as I breathed a little more easily, I felt the mounting urgency of the attack in the rest of my system. My sinuses were now completely solid and swelling further, pressing against my cheeks and eyes. My face, ears, and neck burned, and a desperate itch ran up and down my spine.
I had to get to some epinephrine. Also known as adrenaline, it was what I had been given when I was rushed to the hospital with my asthma emergency. Since then I had been trained to inject myself in the thigh and carried a kit (called Ana-Kit, short for anaphylaxis kit) around with me. Once, during a moderately severe attack, I had given myself a half-dose, just for practice, and it had worked fine: easy to inject, swift relief. I woke Barbara, my girlfriend. She had never seen a major asthma attack before; I knew that it would probably be more frightening for her than for me. From the outside, the sufferer of asthmatic anaphylaxis looks as if he is collapsing inwards, drowning in an invisible sea of himself. “In the car,” I said, trying to show calm, measuring my phrases to fit the amount of air that I could muster. “In the glove compartment. Is my epinephrine syringe. Please go and get it. Right away. Here are the keys.”
Alarmed, she dressed hurriedly and ran out.
The attack was mounting rapidly. By now I had two hearts, one in each ear. The effects of the Primatene had been overrun, and I felt my chest and throat tightening around my windpipe. My upper body had become panic, operating with a life and purpose of its own. I felt as if my intelligence had suddenly separated from a body gone amok and left alone and in charge, like the captain of a torpedoed ship with six deck-loads of passengers and crew milling around and beneath him, screaming, and the engines driving the ship straight down. But the epinephrine would stop all this. Everything would be all right as soon as the epinephrine arrived.
Barbara burst in with the kit, not the half-used Ana-Kit but an ostensibly more sophisticated tool I had been given since, an EpiPen syringe, commonly prescribed for those with potentially fatal bee-sting allergies. When I opened the tube, I saw that to my
surprise it didn’t look like a syringe but a large gray ballpoint without a nib. Press against thigh and hold in place for ten seconds. I did so. Nothing happened. I pressed my thumb against the butt-end; perhaps I had to push the needle in myself. Still nothing. How did this damn thing work? I jabbed it harder against my leg. There was a thudding noise, and I felt the needle ram into my muscle with not a stabbing pain, but that deep, unnerving thump that is the real sensation of a stab wound. I was startled — but at least the epinephrine was going in. Now things would be all right.
To be on the safe side, I waited 30 seconds before withdrawing the needle. As it came out I was surprised first at the length of it — no wonder they keep it retracted! — and then at the sudden rush of blood. This shouldn’t be happening! I cupped my hand under it, yelling for a paper towel. Three fat drops seeped between my fingers and spread into the white cotton rug. Next morning they would be the only visible signs of the night’s events.
Within a couple of minutes it became clear that the epinephrine wasn’t working. Had it all bled out? Had I developed a resistance to it? What the hell was going on?
Asthma feeds on panic; asthma is panic. I breathed from my diaphragm and calculated. The Primatene, unlike the albuterol inhalers, contains epinephrine — 0.3 mg per dose, I thought. I had just injected myself with another 1 mg. How much would it take? What would happen if I took too much?
This is the paradox of chronic illness. The patient grows around the disease, like an oak tree engulfing a barbed-wire fence in its trunk. My own habits and shortcomings probably perpetuate the condition; the asthma disappears under the bark of my character where I am least likely to look for it. The answer, it would seem, is to remain vigilant, to inform oneself of the latest research, the newest medicines — but such vigilance shades into hypochondria; and, more importantly, anxiety brings on asthma. Research suggests that those who worry most about asthma are probablv those who resort most swiftly to the inhaler; and there nothing so terrible as the sight of someone sucking on an inhaler every half-hour, a slave to his own salvation. Breathe slowly, I told mvself; think quickly.
It was an eerie, vertiginous feeling. I was confronting the normally unexamined mechanics of staying alive, like the clock face turning and staring at the movement in the case. What are the most vital functions? Breathing. Heartbeat. Brain activity. Of these only breathing is at all voluntary. The cardiac patient, sensing the onset of arrest, can't will his heart back to its measured beat, soothing it down from a frightening erratic fibrillation; he can’t rip open his chest and squeeze once a second, his life literally in his own hands. Only with breathing are we given the devil’s option, the chance to Keep ourselves going by force of will.
Barbara hovered around me, trying to stroke my neck, asking questions. My irritation rose like the flush in my skin. I did not need love; I needed competence. “In the kitchen,” I told her. “Opposite the sink. Top shelf. Ana-Kit. Orange plastic box. Rectangular. Under the sink. Bottle of alcohol. Get them both now.”
She found the half-used Ana-Kit and the alcohol. I’ve used the needle before, so it will have to be sterilized, reasoned my intelligence, pacing the bridge, though I had no idea whether dipping the needle in alcohol would kill all the germs or whether at this stage that even mattered. I dabbled it briefly, then jabbed it at my thigh. It bounced off. Maybe the needle had been blunted and wouldn’t work a second time? I pushed harder and it slid through the skin as if through linoleum. I gave myself another 0.5 mg of epinephrine. This, surely, would be enough.
I sat on the edge of the bed, naked, hauling in breath, bent over like a coal man hauling his sack. The epinephrine did not work.
I used to live near Accles & Pollock, in Worcestershire, England, the company that according to the Guinness Book of World Records made the thinnest tubing in the world at the time, its bore being a hundredth of an inch or so, more of a thread than a tube. That’s what my trachea felt like. I can get just enough air to survive if I don’t move or talk, if I can focus on the muscles in my throat and convince them not to contract still further. Even so, I realized I was better off than during my first major attack, in 1984, when that thread of a tube filled up with fluid, and I knew what it is like to drown.
I was dimly aware that Barbara was asking, “Shall I call an ambulance?’’ looking anxious. I nodded. My face felt stretched, like Edvard Munch’s screamer. I thought of an elderly woman I once knew who died slowly, losing touch with her surroundings, sinking in on herself, confused, muffled, protected from knowing what was happening as if the body released some hormone that made it all not matter very much. That’s how I want to die, I thought.
Anything but dying fully aware and in a panic.
My head had started aching. By now sharp pains shot through my back whenever I breathed in. Technically, asthma is caused by not being able to breathe out; patients have died with substantial amounts of air trapped in their lungs. It doesn’t feel that way to an asthmatic. Breathing in is inspiration, the grasp for the straw of air. Breathing in is the beginning of life, the first gulp as the diver reaches the surface. No asthmatic works to breathe out.
The fire crew arrived and flitted around like shadows—dark, unimportant, almost unreal. I’ve read that to an addict, nothing but his drug matters; and at this point I knew that this must be true in a literal sense: nothing but the drug has matter. Everything outside me was insubstantial, at most only a distraction, an irritation. Shades of people moved around the room, asking questions I couldn’t answer, murmuring to each other, their walkie-talkies crackling. The only person I wanted to see was the one with the cure, which would give him or her definition and meaning. For once I could see what Sartre meant, we are given not only purpose but existence by our acts. Barbara and the fire crew couldn’t help, so they vanished; I shrank further into myself and worked on giving myself existence by breathing.
At one point the panic rose like a wave and engulfed me. “Help me,” I croaked to one of the fire crew. He stared at me. He doesn’t know what to do, I thought. I shouldn’t have involved him. I turned back into the internal world, where I was needed and could be of some use.
The ambulance crew arrived. “Do you feel as if you’re going to pass out?” they asked. I worked up enough air to talk. “I feel. As if. I’m going to die.” That answer didn’t fit their criteria for an informative response, and at once it became clear that they couldn’t do anything to help me either. But at least we would be off to the ER, which was only a few minutes up the hill.
First, though, they had to get me out of the house. “Can you put your clothes on? Can you get into the chair?” they asked; and when I didn’t answer they thought I was being stubborn or I couldn’t understand them, and they repeated the questions several times. But in the sick man’s solipsistic wisdom, I knew better than they. The slightest movement, even talking, involved constricting some group of muscles, and every muscle was now connected to my chest, pressing on it. I had to plan every movement ahead, to imagine the most efficient, the most graceful way of doing it, then wait half a minute to relax as best I could, make the movement and collapse into myself afterward as my pulse shot up and my hearts pounded in my ears, my thread of air temporarily crushed. I felt like a dwarf— large head, barrel chest, puny arms, virtually nonexistent below the diaphragm. I had shrunk to all that mattered. It amazed me that when I finally half-stood, I was taller than they were.
Once in the ambulance, breathing oxygen through a mask, I hoped the worst was over. In the E.R, the doctors and nurses asked me, “Can you tell us what’s wrong?”; and, astonished and angry that they couldn’t tell that I couldn't speak, I grabbed the pen from someone’s breast pocket and wrote on the paper sheet on the examining table what had happened and how much epinephrine I had already taken. They changed my oxygen mask for an albuterol one, and within minutes my breathing began to clear — a strange sensation, like someone removing thick cobwebs one by one— and I began to notice my headache and nausea. “That’ll be from the epinephrine,” the nurse said, though she had no idea why, if I had so much of the drug in my system, the attack had ridden roughshod over it. She brought me a bowl, into which I threw up, and acetaminophen suppositories, which I accepted with the lack of dignity of one to whom other people barely exist.
I sat on the table for an hour and a half, unwinding, my muscles unwrapping themselves until I was no longer a clenched triangle but could sit back against the pillow as the external world returned. I felt as if I had been inside out. The staff was as surprised that a major attack had passed so quickly as they were baffled about what had caused it. Within two hours I was shaky but breathing normally; at 4:00 a.m. I shuffled out to the lobby in lime-green hospital Styrofoam slippers and took a taxi home.
In the emergency room, as the attack eased away, I wondered if afterward I would have that transformative experience of seeing the world afresh and anew in all the glory that I had been overlooking; then, when that seemed unlikely, I wondered if I would emerge like Coleridge’s wedding guest, a sadder but a wiser man. In fact, I was no wiser at all, as far as I could tell. Instead, it felt as if I had been visited during the night by a bear that filled the room with a blacker darkness for a terrifying long moment and then lumbered out, leaving me wondering how the hell it got in and whether it could return and leaving also a faint but perfectly distinct odor that might be the creature or might be my own smell of panic.
THE SHAPE Of THE LUNGS, you must understand, is significant.
They look like the roots of a tree, perhaps, though far spongier and more delicate. They begin with a single trunk, the trachea or windpipe, running down from the back of the throat, pink and purple, glistening with the fine coating of mucus that catches stray particles of dust, soot, etc., and is our airway’s first line of defense. Below the base of the neck the trachea branches into two bronchi, one for each lung, each of them not merely a rubbery tube but a highly sensitive and complex environment, with muscled walls capable of expanding and contracting to allow more or less air to pass through (less if the air is suddenly cold, more as one exercises) and a highly specialized skin surface, or epithelium, patrolled by the myriad complex agents of our immune systems and studded with goblet cells that release more or less mucus as the situation demands. Each bronchus branches again and again into smaller and smaller airways called bronchioles (miles of them packed into less space than a gallon jug) and they continue branching until, at their tiniest and most threadlike ends, they blossom into a cluster of budlike alveoli, where the miracle of gas exchange takes place and oxygen passes into the bloodstream without blood seeping into the airways.
This is also what asthma is like. It may sound like one disease, but in fact it may have two entirely different primary symptoms: a wheeze or a cough. And the closer one examines asthma, the more it subdivides. Many people associate asthma with allergies, but it isn’t clear why we have allergies or how we develop them or why they strike different people at different ages or why one person’s allergic reaction takes place in the nose and is called hay fever (or allergic rhinitis) while another takes place in the skin and is called eczema (or atopic dermatitis, “atopic” simply meaning allergic), whereas others take place in the airways and are called asthma (or, nowadays, reactive airways disease). But many asthmas don’t seem to involve allergens at all, being brought on by such apparently benign conditions as laughter or exercise or cold air.
The new thinking is that asthmatics have some unexplainable chronic inflammation that leaves our airway walls permanently swollen and hypersensitive, ready to cringe inward at the slightest threat, strangling our air supply. But neither of these branching, diving explanations accounts for the asthma attacks apparently started by moments of anxiety, nor the fact that an entirely different mechanism, involving an enzyme called cyclooxygenase, can bring on some of the most vicious attacks of all and mean that a single aspirin or ibuprofen tablet could kill me.
This branching airway design is a metaphor for one other feature of asthma, in fact. When we look around us for the potential dangers, the items in the landscape that might kick off my asthma or yours or your neighbor’s, they might be lurking literally anywhere. Allergies may bring it on, but the allergens themselves are almost infinitely diverse: ragweed, beer, shellfish, dust mites, molds, cockroach scales, red wine, grass pollen, peanuts, cat dander, and literally hundreds of others. Soot and dust particles may trigger an attack, or cigarette smoke or car exhaust. Thousands of substances in the workplace can be equally devastating: carpet-cleaning fluids, mildew, toluene diisocyanate, mites in grains and flours, chemicals with syllables too numerous to count, let alone pronounce. It is as if our whole environment in California in 1996 were peppered with asthma mines waiting to go off, or possibly the other way around, that our immune systems are alert to an increasing number of threats in a world we are constantly molding to fit what we think are our best interests.
The Centers for Disease Control in Atlanta reported that between 1980 and 1987 the U.S. death rate from asthma rose 31 percent and has almost doubled in the last ten years. In 1992 about 5000 Americans died of asthma. Six percent of all hospital visits are a result of asthma, with asthma-related health care costing more than $4 billion a year. At least 12 million Americans, and 5 percent of all people in the world, have asthma. The death rate for asthma is rising everywhere. Nobody knows why.
Children in particular seem to be at risk, especially black children, especially those living in inner cities. Perhaps a million children have asthma, which is the commonest reason for them to miss school and one of the most frequent causes of their hospitalization. Childhood asthma deaths rise by about 6 percent per year. Hospital admissions for childhood asthma almost tripled between 1970 and 1980, while all other childhood diseases remained stable. The bulk of the total hospital-admission increase was among children, with black children admitted four times more often as whites.
The official line is that asthma is an incurable but treatable disease, and the vast majority of asthma sufferers ought to be able to live normal lives. After a long period of free-for-all, there is now a set of official guidelines for diagnosis and treatment; and since the introduction of inhaled steroids a little less than a decade ago there are now good drugs that should have the whole issue under control.
Yet asthma is not going away.
By the most optimistic estimates, it is as common as ever, and most physicians fear that unlike almost every other disease, it may actually be on the increase. As the ’90s progressed, more and more doctors appeared in the newspapers admitting that the wonder drugs had not turned the tide, and every so often another death from asthma hits the local or national news, creating a small but disturbing ripple of alarm.
The more I find out about asthma, the less I think of it as a disease and the more it starts to seem like an index of dysfunction. No matter what avenue we venture down, sooner or later we run into a provocative silence or a flurry of contradictory answers.
We learn how our car works when it breaks down; similarly, the presence of a widespread chronic disease, incurable despite our belief in scientific medicine, often severe despite the fact that we should be able to control it easily, indicates an entire network of cracks in the smooth facade of our understanding — of disease, of agriculture and industry, of the family, of social welfare and public health, of ourselves. If we knew more about asthma, we would know a darn sight more about ourselves and about the world.
WHEN WE THINK Of DISEASE, we think of doctors, and we think of doctors curing our disease. This doesn’t work with asthma, not only because asthma is incurable, but because a very strange and usually hidden dynamic exists between asthmatics, their doctors, and their medications. In short, asthmatics tend not to see doctors and not to take medications.
This apparently baffling behavior is due in part to the fact that some asthma medications don’t work especially well, and some tend to draw attention to the self-conscious asthmatic. It’s also due partly to the fact that the critical medications for controlling a long-term incurable disease are preventive and need to be taken for life, and we are accustomed to thinking of medication as something we take only when we absolutely have to and resent it. Above all, though, asthmatics need a very particular kind of doctor.
Michael Welch of the Allergy and Asthma Medical Group and Research Center on Granite Ridge Drive in Mission Village is widely regarded as one of the premier asthma physicians in the country. In part, his reputation comes from the cutting-edge research he and his colleagues are undertaking. (Most clinical allergists do virtually no research; some don’t even read the research.) His associate Carol Gallet showed me what the Pentagon would call the new delivery systems. The aim is to get away from Freon and fluorocarbon propellants and to make more use of powders than atomized liquids. She showed me a state-of-the-art med dispenser that looked like a diaphragm case. You cock its release mechanism, trigger it, and it dispenses a measured dose, simultaneously recording on a small counter how many doses are left/have been used — a very useful safeguard against the panic of a severe attack and a virtually empty inhaler.
Dr. Welch’s office is also testing the first nebulized, inhaled steroid. Previously this was a blind spot. Small children have to use nebulizers (like small humidifiers in which the medication is dissolved) rather than inhalers because the latter require a coordinated in-breath as the med is released, which is too complicated for them. On the other hand, the inhaled steroids that would be very beneficial to young asthmatics wouldn’t dissolve easily enough to be used in a nebulizer. Welch’s office has the first prototype to solve the problem with new soluble steroids.
They’ve also created what Welch jocularly calls the Cat House, a trailer in which patients can be tested for cat allergy and try out a new form of immunotherapy involving T-cells.
The niftiest gadget, though, is called Airwatch. It looks like a three-tone stopwatch-cum-Sega game. This was especially appealing to a kid who had just come from being intubated but, as with many asthmatics, had no interest in learning more about his condition or monitoring his breathing with a peak-flow meter. He had been emptying a Ventolin inhaler a week — toking on it every half-hour, eight times the recommended rate. Airwatch is a small computer. The kid programs it with his normal peak-flow readings, then pulls out a small mouthpiece into which he blows. The readings tell him how freely he is breathing at the moment. At the end of a week he flips open a small cap at the base of the Airwatch to reveal a phone jack. He plugs in the phone line and his readings for the week are transmitted to Palo Alto, where the service is based, and then faxed to his family doctor. It’s something of an upscale service and not cheap — $163 for the first year for the Airwatch plus the service and $100 a year thereafter. But all asthma meds are expensive. The important thing is that the boy might actually use it.
Yet probably the most important reason why Mike Welch is so highly regarded by his patients has nothing to do with his research or his professional qualifications; it is that almost immediately you, the patient, realize he is going to be there for you, which, for someone with a chronic illness, is as important as any other feature of treatment. An asthmatic, whose illness is not only chronic but can be very frightening, needs someone to bond to, someone who is both skillful and caring. “The active presence of the physician,” writes Eric Cassell in The Nature of Suffering, “is part of the treatment.”
After my major attack in November of ’91, I was referred to a physician who was generally regarded as a top asthma specialist. He gave me a prescription for Vanceril, some dosage instructions orally and in writing, and told me to come back once in a few weeks, again in April or May, at the beginning of the pollen season, and again in a year’s time. I didn’t go back for the next appointment; I went back several months later and then skipped the spring appointment and one-year follow-up.
I didn’t go back because I just didn’t believe he was sincerely interested in my welfare. “If you have another attack as serious as this one,” he instructed me, “you must see me at once”; but as I was enfolding myself gratefully in his concern, he added, “during office hours on the next working day."
To hell with that, I thought.
When six or eight weeks went by and no receptionist called to jog my memory about the next appointment, I knew. He didn’t care. He was a specialist with a full waiting room. At a rough guess, he made five times my annual salary, yet the sign in the front office still demanded payment in full at each visit. Fuck him. When I did return, it was, though I didn’t realize it, to prove him wrong. He had said I was probably suffering permanently reduced lung function, by implication because I hadn’t come to see him sooner. When I went back, not having wheezed for four months, I blew so hard into the peak-flow meter the needle went off the chart. Take that.
He had done his best, but instead of getting me to follow the precise duplicated instructions he had handed me, he had pushed me — to be more accurate, I had retreated — into the shadows of medicine. And virtually every asthmatic I’ve talked to has had a similar experience, often, sadly, with more than one doctor. Sara Sweet, of the group Parents of Children with Asthma, took her daughter Bonnie to see one of her HMO’s allergists, who showed her glossy pictures of dust mites and then asked, “Well? Any other questions?” The pediatrician was no better. “Lousy. Unsupportive.” She now pays out of her own pocket to see Welch, who is not on her HMO’s roster.
The three most important qualities for a doctor, wrote Sir William Osier, the great turn-of-the-century physician, are availability, affability, and ability, in that order, and for chronic disease at least, that is still true.
This may be even more true for the parent of a severely asthmatic child, as he or she is not only helpless in the face of an attack but also in the face of his or her failure as a parent. She has tried everything she can for her child, and he is still in unpredictable and desperate danger. In those dark times, it is vital to have a physician who is caring for the parent as well as the child.
“You want to feel as if you have someone who can rescue you and rescue your child,” explained Lynn Devine, who now sees Dr. Welch with her son Alex. “Some of the best doctors in town don’t get that.” Before she saw Mike Welch she took Alex to a doctor named Nevin Wilson, who has since left the area. Wilson recognized the value of Osier’s doctrine to such a degree that he once saw Alex at 10:00 a.m. on Christmas Day.
Without someone to bond to, we may do almost anything, trying increasingly desperate alternative remedies, visit well-meaning and likable doctors who know relatively little about asthma (all too common, sadly), or convince ourselves that our asthma is not all that bad anyway, pushing ourselves further and further into the shadows of medicine and setting ourselves up for that final desperate dash to the ER.
Our defiant and resentful behavior is officially called “non-compliance.” I talked to two nurses in San Diego who couldn’t understand why people with asthma keep smoking, don’t take their meds, or leave it until the last minute to come to the ER. “Most people are really, really stupid,” said one. “No, I think people are just lazy,” said the other.
This is quite wrong and shows how wide a gap now yawns between the world of medicine and the world that medicine is intended to serve. Asthmatics “fail to comply” not because we are congenitally stupid, lazy, or stubborn, but because severe asthma causes a double rejection of reason. In the throes of suffocation we don’t want a cool medical intervention, we want someone to cling to in abject terror. (Lacking a doctor, I called, “Help me. Help me," to a fireman, who was as helpless as I.)
“Asthma is such a frightening disease,” said one of the few doctors I’ve met who understood the needs of the asthmatic, “that an asthmatic wants someone to bond to” — and as soon as he said “bond,” I vividly imagined the doctor I’ve never had, a knowledgeable friend, present and comforting. I saw myself bent over, gripping his arm, trying to breathe, knowing that he could be trusted and that I could allow myself to be seen in this moment of panic and weakness.
Which is, of course, the second rejection of reason. Once the attack is over — which may, after all, be only a few minutes later — the disease seems to vanish, and we are left feeling not only scared to the core but also very foolish. It’s as if a tidal wave had crashed in through our bedroom window in Kansas, overwhelming us, taking us to the point of drowning, and then withdrawing without a trace, the carpet not muddy, the bedclothes not even damp. How can we not be ashamed of our panic, our moment of weakness? This makes it all the harder to go to see a doctor when we have no symptoms to justify our poaching of his time, only an emotional residue that is all the more uncomfortable for having no cause that we can show.
His cool professional manner rebukes our desire to blurt out, “Doctor, I’m scared”; and his trained reply, “What seems to be the trouble?” reminds us that this is supposed to be an intelligent exchange of medical information. So he dismisses and we beg for something more, or else our pride tells us we’d rather go with the patent medicines and try to suppress the anxiety, though to do so will lead us to be accused of denial. All medicine is driven and distorted by fear, and asthmatics are merely an extreme case because the condition is so common, so frightening, and so quickly over. Or maybe the ideal of cool professional detachment is simply the wrong model.
ONE COMMON REASON asthmatics don’t take their meds as prescribed is that they don’t trust drug companies — a distrust that is often so deep that it sucks in doctors who prescribe and therefore apparently endorse not only the drug companies’ products but also their actions. Physicians are, in fact, in a very tricky position in being beholden to their pharmaceutical cousins while having virtually no control over them. Quite the reverse, in fact; the drug companies are not above trying to mislead doctors — indeed, they must impress their products’ effectiveness and reliability on the doctors who will prescribe them or use them in hospitals.
You’d imagine that in the professional periodicals, at least, drug companies would be kept to the straight and narrow, but a 1992 UCLA study of 109 ads in 10 leading medical journals found that 100 contained “deficiencies in areas for which the FDA has established explicit standards for quality.” Forty percent of the ads reviewed exaggerated a drug’s benefits or downplayed its known hazards; 30 percent cited statistics from “inconclusive, dissimilar, or poorly designed studies”; and 30 percent included misleading graphs or tables. If these are the ads directed at those most likely to spot their errors or liberties with the truth, what chance does that leave the muddled layman who is still at the kindergarten level of trying to spell “relief’?
It leaves us watching television news, but there too the drug companies have exerted their influence. A notorious example was the Billie Bloom videotape, which looked like a locally produced spot in the evening news, which aired on KGTV, Channel 10 in San Diego and in other cities in early 1987. Actually, it was a “video news release” produced by a public relations agency in New York, nominally on behalf of the Asthma and Allergy Foundation of America but paid for by Key Pharmaceuticals, a contributor to the foundation and maker of a drug that got a favorable mention in the tape. Billie Bloom, an 11-year-old asthmatic, reenacted on camera an asthma attack that occurred after she had switched medicines. The thrust of the message was that generic drugs can be less safe than brand names — a message that the FDA considered misleading, but it took no action. In all, the New York Times reported, the tape was aired 31 times by 23 stations and was seen by an estimated 1.3 million people.
ONE OF THE MANY MIRAGES CAUSED BY ASTHMA is the belief that if we look at what helps the condition, we may better understand what causes it. The trouble is that over the centuries sufferers have been lured by a wide variety of so-called cures, and astonishingly, many of them have done at least some good. In a sense, asthma is the perfect advertisement for a holistic approach, because any improvement in what is now called “baseline health” tends to lessen asthma symptoms. Or maybe it’s the other way around: asthma, or at least some asthmas, is an illustration of our general health —as a person, as a society, as a planet.
An Egyptian asthmatic of the 16th century B.C. might have been handed a papyrus prescribing boiled and strained colocynth, onion, goose fat, beer, and decayed flesh. Chinese remedies included dried geckos and tea made from cockroach entrails. In fact, many traditional Chinese acupuncture herbal remedies involve making a small beetle eat the herbs and then eating the beetle. In classical Greece it was thought that sulfur, which induces coughing, would help asthmatics cough up whatever was making them wheeze, so kindly guides led asthmatics up to the crater of Mount Etna to inhale the fumes. American folk treatments have included licorice water, apple water, mullein, gum ammoniac, vitamins, cider vinegar, marijuana, and cocaine. Asthmatics have been sent to clinics at the tops of mountains and in the depths of salt mines.
I myself have had desensitizing injections, preventive medications, steroid shots, psychotherapy, and even a course of injections of tobacco leaf, silver, and blackthorn prescribed by a homeopath and gingerly administered by my girlfriend, who was understandably reluctant to jab me in the back of my neck.
Perhaps as many as 80 percent of asthma sufferers have tried a non-mainstream treatment at some time. Our faith in alternative medicine echoes the creed of an earlier doctor. Sir Arthur Conan Doyle: when you have eliminated the impossible, whatever remains, however improbable, is the truth. If Western medicine says asthma is incurable, we’re straight off into the realms of the improbable, sniffing along the trail laid by none other than Sherlock Holmes. This is a logical fallacy, of course — just because orthodox Western medicine has no cure, it doesn’t mean that anyone else does either. But if the local MD can’t do it, then it takes no more than optimism to ferry us into the colorful land of the unlicensed and the unproved; and the hooting derision of the crowd in the white lab coats standing on the shore behind us makes us only more determined to prove them wrong.
In San Diego, I decided to investigate three that were still relatively unfamiliar to me: hypnotherapy, yoga, and acupuncture.
JUST WHEN TOU THOUGHT ASTHMA WAS SIMPLY a matter of allergens and inflammation and could safely be left in the hands of the allergists and immunologists who understand antibodies and chemotactic mediators, Dr. George Pratt of Scripps Memorial Hospital and UCSD includes in his book A Clinical Hypnosis Primer the statement, “By current estimates, 50 to 80 percent of all illness is psychosomatic rather than organic.” This does not mean they are self-inflicted or “all in the mind.” It means that “strong emotional states or unconscious psychological conflicts can in time cause organic symptoms or exacerbate existing organic pathology.” In short, he says, stress can produce just about any physical symptom we can imagine.
Exactly how hypnosis works is something of a mystery, he concedes. The American Society of Clinical Hypnosis has written, “None of the definitions of hypnosis satisfies the criteria for a good scientific theory.” (When I read that I cackled with glee and rubbed my hands together. Exactly the same is true of asthma.) All the same, in 22 years of using hypnosis as a psychotherapeutic tool, he has found it frequently very helpful in treating people to relax, to feel in control, to reduce the frequency and severity of attacks, perhaps by reducing anticipatory anxiety and the fight-or-flight response that sets off the immunological cascade that feels like panic.
His most successful patient, though, was himself. In the early ’80s, at a time of enormous personal stress, he developed adult-onset asthma serious enough to leave him unable to run or take part in sports and to require daily Prednisone and a variety of other meds. After some time he realized he might try some of his own techniques for his own benefit.
“I was so panicked over this I hadn’t thought of doing what theoretically I knew I could do.” He set aside half an hour twice a day to practice self-hypnotic techniques, listening to relaxation tapes that he devised for himself, imagining his niascles getting heavy, feeling comfortable, picturing pleasant scenes, his body beginning to heal, breathing better. He also set up a cue to trigger this relaxation and got to the {joint where he only had to take a break from whatever he was doing, relax his neck and shoulders, and touch his thumb and forefinger. Ten years later he is completely free of asthma symptoms; his chief of staff. Dr. Adrian Jaffer, a renowned allergist, can’t believe it.
The success of Pratt’s hypnosis shows the strange inter-knotted cause-and-effect in asthma. For many asthmatics — but not all — one of our most frightening experiences is that of a severe asthma attack. If fear can provoke asthma, then, fear of asthma can provoke asthma. By extension, anything that mimics asthmatic symptoms can potentially have the same effect, though such facsimiles vary widely from person to person. For years I started wheezing as soon as I swam underwater, as if the sensation of pressure on my chest were a threat in itself or a threat of a threat. (I can’t stand clothes that are tight around my neck either.) A friend is sensitive to rooms with low ceilings, as if physical claustrophobia were a reminder of the internal claustrophobia of asthma. Maybe this is why some of us even seem to be sensitive to changes in air pressure.
This is called “one-trial learning,” Pratt explained. “Anything that reminds you in the least triggers a biological-psychological event.”
This is why, he said, panic attacks and anxiety disorders respond so well to hypnosis. “If you can change the message you’re sending yourself while simultaneously relaxing yourself, you can make a harmless process out of going through an event that would normally elicit a tremendous response.”
Who knows how far afield we scan for such danger signs? Being trapped in an elevator has virtually nothing in common with the physical experience of an asthma attack, yet the fact that we asthmatics instinctively talk of our physical experience in terms of claustrophobia, and the claustrophobe talks of feeling as if he can’t breathe suggests that we feel (the very word has both meanings) in both dimensions. In my phone conversations with my ex-wife, I felt trapped, helpless, unable to speak my mind, forced to hold my breath in the hope that the threat would go away. Is it too fanciful to suggest that in doing so I was creating an emotional-physical landscape that was all too reminiscent of asthma, setting off my own alarm system?
A note: Pratt writes that “a hypnotic suggestion is only effective to the extent that it is accepted by the patient.” The proof of a drug, on the other hand, is that it works irrespective of the patient’s will, and we have come to believe that (1) drugs can cure anything, and (2) because they don’t need our help, we don’t need to make any adjustment in our attitudes or behaviors. We have externalized the responsibility for health and cast it in pill form. Yet this leaves us with profoundly ambivalent attitudes to medicine, as the phrase "a bitter pill” reflects. We want the immediate cure, the magic shot, yet we are terrified of the needle. We want the miracle cure but despise the drug company.
Nowhere is this better illustrated than with asthma, where the miracle drugs — the inhaled steroids — arrived at the beginning of the decade with a loud fanfare that became increasingly muted as asthma continued to flourish. The fact is that drugs, too, are largely dependent for their effectiveness on the patient’s acceptance. If we don’t believe in our meds, we simply don’t take them, or don’t take them properly, or often enough. Meds, like a good diet and regular exercise, must be part of our desires and habits if they are to do any good. The future is not pharmacological.
LINDA ROBINSON DEVELOPED ASTHMA during a bout of pneumonia five years ago. Thereafter, whenever she became anxious or upset, especially during family conflicts with her daughter, she found herself wheezing heavily, unable to finish a sentence. She also wheezed whenever she had a cold or respiratory infection or with exercise.
Six months later she started attending yoga and meditation classes at the Vogel Institute in San Diego. “Almost immediately I noticed a difference. I could stop an attack in the middle.” While arguing with her daughter, “I’m fighting for air, and she got really scared, and she’s freaking out, which helps (the asthmaj escalate even more. Right in the middle of it I was able to relax and change my breathing, so I was breathing diaphragmatically and under control, and after a few minutes my breathing was back to normal.” She still uses her inhaler when she gets a cold, but otherwise she has barely wheezed since.
Yoga has generally good press among asthmatics, but I had never given it a real try, because the only time I took a yoga class I got bored. I decide to give the Vogel Institute a call, and one Thursday evening I find myself in an airy, high-ceilinged room under exposed beams, taking a yoga class with Ken Temple.
The institute, he explains, essentially works on stress reduction and breathing techniques. Yoga, meditation, and deep relaxation, then a breathing technique called prana yama, or the superoxygenation breath, to give more control of breathing, less sense of panic. More esoterically, they teach alternate-nostril breathing, “a way to fine-tune the body’s neurological system.” The spine has two energy systems, he said, one of which arrives at each nostril.
“One heats the system up, the other cools it down.” Breathing with alternate nostrils in a specific way, he said, helps balance the two systems. “The breathing goes to the reptilian brain. It really gets into there, deep and old.”
This sounds pretty esoteric, but the basic concept — breathing from the diaphragm — is familiar to Western medicine.
Many respiratory nurses teach children to breathe from the diaphragm, which lessens the strain on the chest, neck, throat, and back and thus gets more air in with less muscle fatigue and less consequent increase in tension. I can remember relaxing out of asthma attacks up until the age of about 21; after that they seemed to take a firmer grip, and only meds would work.
On the mat, I find that the breathing and stretching loosen up mucus I didn’t know was there, relax muscles I didn’t know I was clenching. I sniff, clear my throat, settle more deeply into the mat. Old injuries reappear in short, sharp twinges; I had no idea I was still guarding them with such silent vehemence. Find the source of the tension; reassure it; relax through and past it. Gone.
Stretching muscles breaks up knots, allowing blood to bring in oxygen and begin healing, flushes out the lactic acid that burns. It releases memories, too. I am 24 again, hunched over in a locker room after a game of squash, feeling the crawling sensation at the base of my throat, trying to release it, feeling with each exhalation the unnaturally long final tapering-off. Don’t fight to breathe in again too soon. Draw down the diaphragm as if it were the bottom of a balloon, pulling air into the lungs without having to use the chest muscles, because they are the ones in trouble, already cramping and twitching, tense, exhausted, sending small stabbing pains between your shoulder blades. Draw down the diaphragm. Let the breath go, slowly, taking its own time. The last few inches of air take forever, but don’t be afraid. Don’t clench. Don’t worry about the wheeze, almost musical at times like a discord on a tiny electric organ. The last few inches of air take forever.
Relaxation is an acquired skill. We are overtly taught how to be hasty or dutiful, how to fight or to grin and bear it, but not how to focus on a particular muscle and relax it. Which is unfortunate, as relaxing is intimately connected to self-knowledge, discovering the body from inside out and thereby discovering the mind and its unexpected quiet authority. After I developed asthma at the age of 11, my mother taught me a few of these tricks, working down the body, focusing on each muscle group in turn, but I suspect she was unusual in this. If you try to force a muscle to stretch, Ken says, it resists — and I’m thinking muscles are like asthma patients, resistant, noncompliant. Fear is stronger than good intentions.
“Asthma is simply a habit of fear, a pattern that can be discarded,” Temple says after the class. “That’s why there is a real cure for asthma in this program. It takes care of that underlying fear.” Everybody has fear, he adds; different people express it in different ways. The crucial thing is not to accept that crippled posture, that crippled self-image, “knowing that our real identity is not the disease.” (He is one of a number of people who believe that to call oneself an asthmatic or an alcoholic is not an acceptance of responsibility for one’s condition but a dangerous tarnishing of one’s own identity.) "We are not isolated beings but are connected within ourselves, with each other, and with the universe.”
Later, a couple of echoes come back to me. Erhard Vogel’s Expert in Life program sounds very much like the advice that physicians who work with chronic illnesses such as asthma and multiple sclerosis give their patients: become an expert in your condition. The take-charge attitude that Mike Welch advocates reappears here, only writ larger and broader. Take charge not only of your illness but of your life in general. It’s a sign of how disease-focused Western medicine has been that we have swallowed this perspective. How can we take charge of a disease without addressing the rest of our lives? This is one of the central problems of asthma. Monitoring my symptoms with a peak-flow meter is indeed one step toward understanding and taking charge of my condition. But how much good does it do if I am stuck in poverty or addicted to cigarettes, or my parents won’t take my illness seriously, or my husband is an alcoholic, and it’s all I can do to keep myself intact?
I can’t speak for Erhard Vogel’s philosophical and therapeutic approaches, having seen virtually nothing of them, but I can’t see how yoga itself can do anything but good — unless it becomes too soothing and we use it as a way to ignore learning about our disease. (It’s all too easy to take Ken Temple’s “Asthma is simply a habit of fear” at face value, nod, and remain in near-total ignorance about what triggers our illness.) Many practitioners of Western medicine are open-minded enough to recommend yoga as part of an asthma treatment; their fear, and mine too, is that their Eastern counterparts won’t grant them the same respect. Taking charge of chronic illness is very difficult without taking a broader grip on one’s situation in life. But taking charge of one’s life should also involve learning about one’s illness, moving back and forth between Eastern and Western approaches with ease, speaking both languages.
George Pratt and Ken Temple use different techniques toward a similar end. Some may work better for some patients, others for others; the degree of belief, in itself, may affect the degree of commitment, of relaxation, and therefore of response. We’re in gray areas here, impossible to quantify. No wonder allergy, with its precise numbers of IgE antibodies, seems so much more credible, so much safer. Whether alternate-nostril breathing really purifies the anabolic and catabolic motor fibers in the spine (as the Vogel Institute literature promises), I can’t say, being a novice.
I didn’t do it. In general, this stuff is impossible to quantify. How much benefit did I get from it, on a scale of I to 10? How much did the guy next to me get out of it? How quickly did it act? Why didn’t I respond as well to yoga when I first tried it 15 years ago? Can the instructor guarantee that his results are reproducible? Are they more effective than placebo in double-blind crossover trials?
(Yet even in conventional medicine, one patient is said to “respond well” to a drug, while another responds less well; we all have different tolerances and different side effects to differing degrees, and when one starts to include the mysterious power of the placebo effect, this yoga stuff is not so weird after all.)
On my way home, I encounter a couple of nurses from Children’s Hospital. They see a lot of asthma: in-patient, ICU, ER. It’s a terrifying thing, they say — for the patient, for the family, for the caregiver. The staff can administer the meds, but then all they can do is watch. Everyone is tense; the families, too, can hardly breathe. The patients are usually silent, hunched over in the classic tripod position, unless they’re very young. The meds make the two-year-olds ballistic, they say, the heart rate way up. Then they may crash, suddenly, their respirations rate dropping like a rock, and then it’s time to intubate them. But this is a last resort. The tube itself is invasive and can make the airways clamp down still harder. And in any case, the respirator tends to work only one way; the positive pressure forces the oxygen in, but there’s no corresponding pressure to force the carbon dioxide out. Asthmatics die with their lungs full of trapped, stale air. This is what we talk about over pad thai and red curry, this and their plans to get away from their work, to visit Australia for a month, to visit the chateaus of the Loire Valley.
THE AIR Of TAI-MAN WANG'S OFFICE IN CLAIREMONT is thick with the strong, barky smell of a thousand herbs. On his desk, under a hundred or so papers, he finds William Chang’s Catalogue and Reference Guide of “Jen-on ” Chinese Herbs and Formulas and shows me some of its descriptions of various asthmas and the recommended remedies. On his shelves stand a collection of mysterious jars of apothecaria and a remarkable range of books in both English and Chinese, books about herbs, about standard Western medicine, a translation of The Yellow Emperor’s Classic of Internal Medicine, which includes what is thought to be the first recorded description of asthma, and, as if to complete the trilogy of alternative cures. Helping Yourself with Self-Hypnosis. I seem to have come full circle.
Wang grew up and trained in Taiwan and came to the U.S. in 1970. He diagnoses by looking at the tongue, reading six pulses on each wrist, palpating key points, testing sensitivity to heat and conductivity. He thereby arrives at a holistic picture of the patient’s general health, the overall flow of his chi energy (a combination of the nervous system plus the electromagnetic closed-circuit system among the tissues, the wired and the wireless) through the meridians that serve the major organs. The flow of energy is regulated by inserting and manipulating needles to stimulate or suppress it. He begins to treat the most acute conditions, then moves on to restore and maintain a general balance of health, both physiological and psychological. Treatment is with needles in the office, with herbs at home, traditionally in tea form, now available as capsules.
He shows me a needle, then with a swift and unexpected flick of the wrist he inserts it into my arm, on the outer curve of the crook of the elbow. It doesn’t hurt as it goes in — a slight shock, perhaps — but after a moment it seems to expand and take up more space, to affect an area roughly the size of a tennis ball. This region feels slightly uncomfortable, a dull ache with an overtone of annoyance, like something that needs to be taken care of but has been put off as long as possible.
As the interview goes on, I find myself clearing my throat every few minutes and am a little embarrassed, then think, screw it. I’m an asthmatic. I produce more mucus than some people. If he can’t deal with it, then he doesn’t deserve to be a doctor.
Two days later I recall this and realize that I don’t clear my throat like that all the time — in fact, the looseness of the mucus started shortly after Wang inserted the needle in my lung meridian and lasted for perhaps half an hour. Have I, in effect, received the beginnings of an acupuncture treatment without even knowing it? My mind boggles, uneasily.
Meanwhile, he reassures me that he refers emergency cases of asthma to the HR, recognizing the need for extreme measures in extreme cases, and advises asthmatics against eating anything cold, such as ice cream, whose temperature “affects the energetic system and delays the recovery.”
In Western terms, these techniques simply shouldn’t work. Some are untested, some unproved, some based on principles that we claim don’t exist. Which is why I am particularly interested to meet Alex Morales, one of Wang’s patients, and his mother, Martha. Before our meeting, she types a two-and-a-half-page letter explaining her ordeal with Alex’s asthma.
I meet them at Wang’s office. Alex does not look like a sufferer. Now 14, he shakes hands firmly, looks relaxed and fit in sneakers, shorts, polo shirt, with longish dirty-blond surfer hair. He starts on the soccer and football teams at Francis Parker School.
Alex suffered his first attack at nine months, Martha says, reading from her account, when the family was living in Phoenix. “I have been blessed with good health, stamina, and vigor all my life. At that time I could not have imagined how his illness would impact our lives.” Over the next five years Alex took Alupent, Bronkosol, Slo-bid, Prednisone, theophylline, epinephrine, Ventolin, and other drugs. “It has been ten years since he took those drugs, and I still remember their names.” He was twice hospitalized; he suffered from accelerated heartbeat, bronchitis, sinus infections, and pneumonia. “He was sick every month for the first 5 years of his life.... He has gone through seven or eight cycles of antibiotics every year for at least 7 years. At age 14 he has taken more antibiotics than I have in 41 years.”
The worst and most constant symptom, Alex adds, was his blocked nose. “It was like I had two pieces of marble shoved up it. I couldn’t sleep well. Phys ed was a no-no. To keep up with my friends when they were running around the playground was hard also. I had to chew with my mouth open, and some days even to talk was hard.”
In 1986, she goes on, she turned to alternative medicines in an effort to wean Alex from the 15 or 20 pills he was taking each day. Over the next six or seven years, Alex submitted to tea of catnip, conifrey, lobelia extract, castor oil packs on the chest and back, glycothalmine in water, steam treatments, Mother Earth cough syrup, massage, postural cupping, herbs of fenugreek and thyme, and chiropractic care to free up the nerves to the nose.
“The beet juice was the worst,” Alex interjects. “It was horrendous.”
“He submitted to everything I did to him,” Martha replies, “but if he had a choice between beet juice and dying, I think he’d rather die.”
She eliminated all meat, dairy, corn, soy, orange juice, artificial coloring and flavoring, sugar, and salt from his diet, then gradually reintroduced each to determine their effects. An allergist said that he was allergic to olive trees. A CAT scan showed nothing wrong with the structure of his skull.
The Morales family had and still has no health insurance. “I have paid out of my pocket for everything,” Martha says.
In the fall of 1995, the Morales family moved to San Diego. “He is now 13,” Martha reads, “and still does not breathe through his nose. Alex has come to accept it. He says, ‘Mom, that is just how I am.’ I say, ‘No. We are treating symptoms and not solving problems.’ He gets sick again. It is now October of 1995. My husband saw Dr. Wang’s ad in the newspaper. I call Dr. Wang. It is 11:30 at night. He answers the phone. Says to bring him in tomorrow at noon. We go. [Dr. Wang) is wonderful. We go 12 times or so, and Alex finally breathes through his nose, slowly at first but then more openly. Dr. Wang has to send to China to get a very specialized medicine to help him.”
On New Year’s Eve, Martha reads, she toasted her son, saying that this would be the first year of wellness in his entire life. “Alex no longer takes any medication at all, thanks to Dr. Wang. God bless Dr. Wang,” she finishes and bursts into tears.
Alex explains that his first impression of acupuncture was not the weirdness of the treatment but the kindness of the doctor, the care with which Wang explained his treatments, the fact that he was going to treat the problem rather than the symptoms.
“It doesn’t hurt,” Alex stresses. He lies down on something like a massage table, Wang positions the needles, sets an electromagnetic lamp over the table to warm the needles, and Alex relaxes. The whole treatment takes an hour to 90 minutes.
He now sees Wang every three weeks. He hasn’t had an infection in four months — a record for him — and he hasn’t used his bronchodilator in two months. New Year’s Eve, a time when he was usually battling bronchitis, he went ballroom dancing at the Marriott Marina with his mother and stepfather.
“You know how some men have a worn patch on the back pocket of their jeans where they always carry their wallet?” Martha asks. “Alex had a worn patch shaped like his inhaler.” Now she looks at his jeans, she says, “and there’s no worn patch. Are they really Alex’s?” She starts crying again.
“If he wanted to marry a girl who had asthma. I’d tell him, ‘Think of her asthma as being like schizophrenia. Now do you want to marry her?’ It changes your life. It changes your whole life.”
A recent issue of the newsletter “Asthma Update” passes on the experience of a doctor from Louisiana who used to treat various pain problems with steroid injections in the upper back (to be precise, in the infraspinatus muscles of the infrascapular fossae). He was surprised to hear that those he had treated who had previously suffered from asthma showed sudden and complete remission. Intrigued, he began examining this area in his asthma patients and discovered that almost all of them found it painful. Was it possible that he had stumbled across an acupuncture point and the injection had in effect acted as an acupuncture needle treatment? Sure enough, there are lung acupuncture points in the vicinity.
In a letter to the journal of Family Practice, the physician reports that he offered steroid shots in the upper back to all his asthma patients and “their asthma was put into instant remission. They no longer wheezed or required ongoing medication and inhalers to breathe. Were they cured? Well, if you use the same standard as for cancer cure (five years without a recurrence), then yes, you must conclude that these asthmatics were cured of asthma.”
If I had a hot dinner for every miracle cure that patients and physicians had told me about, I would be a chubby man. (Blue-green algae was probably the weirdest.) All the same....
OVER THE WEEKEND I TRAVEL DP TO THE MOJAVE DESERT, north of Los Angeles, with the UCSD Cricket Club. This is a paradox, of course. Cricket is played on a grass field, so what are we doing in the land of B-2 bomber bases, bare red mountains, and Joshua trees? The answer, of course, is irrigation, to which the whole city of Victorville, home of the High Desert Cricket Club, is a tribute. We play in the residential development beyond the golf course, next to the artificial lake.
Desert is hypoallergenic: virtually no pollen or mold spores. The clean, warm, dry air is one reason people move here from the damp Northwest and the chilly Northeast. Irrigation — an entire lake, for Pete’s sake — introduces water vapor, which takes whatever airborne allergens are around and holds them in suspension, an aerosol, just like the nebulizers that asthmatics use, perfect for inhalation. Water permits the spread of suburbia, with its lawns and shade trees, and the result is pollen counts and allergic activity utterly abnormal to the region. A number of former desert communities have passed legislation limiting the height to which Bermuda grass may be grown in an effort to limit its seeding and pollination and have even banned mulberry trees, but these are Band-Aid measures.
Irrigation also permits farming, a major source of asthma problems caused by pesticide spraying, but also by more natural causes. “There’s a lot of mold growth that you don’t get in a real desert but you do get in an irrigated desert,” explains Dr. James Ellis, who has been seeing most.of the pediatric allergy cases in the Imperial Valley for 30 years. He sees a lot of children with mold allergy, and the year-round growing season allows no relief from pollen. “My roses — I’m having a heck of a time cutting them back because they won’t stop blooming,*’ he says. Perhaps because of the mild climate, the RSV virus, an especially nasty respiratory virus, also flourishes all year round, irritating airways and triggering asthma.
El Centro has other problems, too, adding up to the characteristic asthma fingerprint distinct to each region. With a prevailing west wind and the city lying in a bowl, below sea level and at the foot of the mountains, El Centro suffers common temperature inversions. When farmers bum field stubble, the smoke often rises about a hundred feet and then moves sideways. This traps smog and pollens that might otherwise disperse. Moreover, winds often blow down from the mountains, bringing pollen from a variety of trees and vegetation higher up. A lot of children are allergic to trees not actually found in El Centro.
Then again, El Centro shares the valley with Mexicali, perhaps ten miles away, where the pollution levels are considerably higher, thanks to emission standards that are more lax than California’s.
After the cricket match in Victorville, played in the brilliant light and limitless visibility of the high desert, we head back in the mid-afternoon. As we wind down the blighted lunar valley toward San Bernardino, the sun is already setting over Los Angeles in a swirl of livid red-purple smog, dwindling long before it reaches the horizon. By 4 p.m., the mountains a mile away on each side of the road are virtually invisible in the filthy air. Heading down into the approaches to the city seems like going underwater, the skinny palms and billboards of the drowned city sticking up motionless into the gloom. The only time I have seen air like this was in photographs of the towns surrounding Mount St. Helens immediately after the eruption.
In the van, my nose begins to itch violently even with the windows closed and only a skylight open a crack. Those of us with slightly tuned-up immune systems, with asthma or allergic rhinitis (alias hay fever) are canaries in the mineshaft of human progress. Any human intervention in the natural world can affect the atmosphere, which is both our most volatile and our most vital medium. The sensitive tissues that come into contact with the air — the delicate linings of our lungs and nasal passages — are constantly presenting us with environmental impact statements we didn’t think to require beforehand.
THE FUTURE FOR ASTHMATICS LIES IN EDUCATION, that subject with which Americans have such a love-hate relationship. A number of doctors have admitted to me that the profession in general does a worse job of teaching parents about asthma than about any other chronic and severe childhood illness. Look at diabetes, for example. If a child is diagnosed as diabetic, the entire family goes straight to the hospital and doesn’t leave until (in theory, at least) they know what the disease is, how to administer the insulin, and what will happen if they don’t.
Many asthma specialists would like to see such aggressive treatment for even mild asthma: but asthma, which is far more common than diabetes, presents a trickier exercise in education. Instead of one shot a day, the child may need three or four doses that, if a nebulizer is needed, require a parent to sit with child in lap for up to a quarter of an hour. Instead of one medication, the pediatrician may have to prescribe two or three, and the sheer process of discovering which medication works best may take six or nine months, during which time the parents become convinced that the doctor is either incompetent or using little Joey as a guinea pig for shady pharmacological experiments. Meanwhile, the asthma may go underground for days, weeks, or even months, making it hard to decide if a course of treatment is working or — this will occur to parents — is even necessary.
Diabetes is simpler. Administer the insulin or your child will go into a coma and may die. Nobody knows when or if disaster will strike an asthmatic; yet even if everything seems okay, the same vigilance must be maintained, the same preventive meds taken. It’s hard to educate under these circumstances, this lack of clear and present danger, and of course the health insurance companies demonstrate their usual don’t-look-at-us attitude by refusing to reimburse physicians or patients for time spent on prevention.
“You see the physician for maybe ten minutes if you’re lucky,” said Mary Beth Parr, currently in charge of asthma education for the Sharp Center for Health Promotion. “They schedule 15-minute blocks for revisits.” When she worked as a nurse in a clinical practice, “I always wanted to take more time with the patients and get to know them on a more personal level, but I was told, ‘Come on, you’re taking too long. I only want you to take vital signs.’ ”
The office was well aware that physicians are not reimbursed for the extensive counseling that a new asthmatic n£eds. The entire frustrating circumstance challenges our understanding of “treatment,” which by implication is swift, diagnostic, and pharmacological. Fifty years ago, with infectious medicine, that may have been true; treatment now needs to involve the active participation of the patient, which means a much higher degree of self-understanding.
And offering education is no guarantee that people will be educated; in fact, the best way to keep a secret is to yell it out loud at an asthma education session. You’d think, for instance, that those with severely asthmatic children would want to get together to share war stories, get tips, draw sustenance from watching others coping. Yet even though Sara Sweet sends out fliers about Parents of Children with Asthma to 2000 patients, the largest meeting was attended by only 22 people; the average is 10 or fewer. Mary Beth Parr has been running one adult and one children’s group per month for a year and a half and has had to cancel more groups than she has run. The largest attendance was 9; perhaps 30 in total have come in 18 months. “Asthmatics think they know everything,” she said. “They don’t see they have a need for additional education.”
The place it is easiest to sell education is in schools; which is just as well, as school populations are rife with asthma. Nationally, 10 million school days are lost each year to asthma. It is the most common cause of missed school days, of children’s visits to the ER, just as it is the number-one cause of hospitalizations for chronic illness and one of the leading causes of work days missed by adults. In 1991 the number of schoolchildren medicated for asthma in San Diego city schools, according to the American Lung Association, was three times higher than those medicated for attention deficit disorder and seven times greater than any other condition.
One in 20 children in San Diego and Imperial Counties, some 47,000 kids, have diagnosed asthma; the total number afflicted is probably double that, because (as in the population at large) those who are least likely to be counted — the poor, the elusive, the immigrant — are most likely to suffer from asthma. Several schools, especially those with a high concentration of military kids, have twice the rate of diagnosed asthma, though this may be a good sign. At least military families have access to health care, and the problem is more likely to be noticed.
Other schools — five in particular, all lying just south of Highway 94 — may have more asthma because the students fit the demographic profile of those at greatest risk. Inner-city blacks and Hispanics everywhere suffer asthma two or three times more severely than whites and Asians.
Schools present a particular series of challenges to asthma care. “Some of the schools are very, very unhealthy environments for asthmatics,” said Janet Wilson, a respiratory therapist at Children’s Hospital, who has aided asthma-education programs in several schools, “and the staff have no instruction in how to improve the situation, and possibly no budget.” Some schools in San Diego don’t even have soap by the sinks, even though hand-washing is a crucial step in preventing the spread of colds and respiratory infections, which in turn are a primary trigger for childhood asthma. Few educators know how important it is to reduce the dust in a school or that industrial cleansing agents may act as asthma triggers.
Moreover, especially in an era of education cuts, schools aren’t set up to give asthmatic children the regular, informed supervision they need. “Getting them treatment on a regular basis is virtually impossible,” said nurse Mary Margaret Loehr, “because in school they’re on a desert island medically.” If a school is used to dealing with medical matters at all, it is used to responding to crisis — the bandage for the cut knee, the quick trip to the ER. But asthma treatment is really about prevention, so every asthmatic child needs a safe and knowledgeable authority figure to look after his medication and make sure he takes it correctly (perhaps 90 percent of children don’t know how to use their inhalers properly) and at regular intervals. Who is that authority figure, if the nurse’s job has been cut to one-third time? When do those medicine breaks take place and where?
Some parents refuse to believe their child is sick and won’t let him or her take an inhaler to school. Some San Diego school districts have no full-time nurse, so the inhaler has to be kept locked up, and the kid has to get someone to open the nurse’s office, which takes precious time and stigmatizes the child. Again, the inertia is against the asthmatic, an outsider, aberrant.
Still, in San Diego it’s not as bad as it is in New York, where in many districts the cuts have eliminated nurses altogether and no meds of any kind may be kept at school. I met a mother who, when her young son had an attack, got a call at the homeless shelter where she lived and had to pick up the inhaler and the baby and walk two or three miles to school.
And yet the most conspicuous signs of hope for improvement are also to be found in the schools, specifically in a program run by the American Lung Association called Open Airways for Schools.
Open Airways grew out of a project developed by Columbia University’s College of Physicians and Surgeons in the late 1980s. “They saw the number of children with asthma coming into the clinic was skyrocketing, and asthma morbidity was increasing,” said Lynn Devine, director of school health programs for ALA of San Diego. The program was designed to reach children at risk who may not normally see a doctor, may not know they have asthma, and may not in fact know anything about asthma at all. The curriculum Columbia developed eventually evolved into posters, handouts, and six 40-minute lessons intended to teach kids that asthma is treatable, that'it does not have to escalate into crisis, that prescribed medications should be taken at the first signs of asthma or cold symptoms, and that children with asthma should live as normally as possible.
When the Columbia team tested Open Airways in New York City among children aged 8 to 11, it found that the children who had completed the program had fewer and less severe asthma episodes but also that their grades improved when they took steps to manage their asthma. Parents reported that they had become more involved, and children without asthma were more willing to help their afflicted peers.
The San Diego Open Airways program started in April ’95 and has rapidly become one of the most successful in the country. “Ninety schools in the first full year of an Open Airways program is remarkable,” said Lynn Devine. Most regions hope for between 10 and 30. The reason, she believes, is that it is run not by a physician but by someone who has learned about asthma through bitter personal experience.
Devine’s second child, a boy, came home from the hospital as a newborn wheezing, although he was six months old before a doctor would diagnose asthma. Now aged six years, he has a variety of severe but maddeningly capricious allergies, has been frequently in hospitals, and has taken a whole basket of meds. A friend once said, “This is like having a disabled child,” but it is possibly more frightening than many more stable disabilities, with its sudden attacks, its dangers lurking in everyday guises — cinnamon toast — the frequent life-or-death rushes to the ER. As a result, Devine has a passionate concern that the school nurse may lack and also knows what can now be done to help even a severely asthmatic child.
In one school she saw a child who was in obvious difficulty. “When the teachers said, ‘Oh, he’s always like that,’ I was able to say, ‘I have a severely asthmatic child at home who has been written up in medical journals because his asthma is so severe. I know what a severe asthmatic is supposed to be like, and if I brought him in you wouldn’t know he was a severe asthmatic.’ ”
Mary Beth Parr is one of many nurses, respiratory therapists, firefighters, and volunteers who took the Open Airways training. Last November she ran a six-week Open Airways course at the Silver Strand Elementary School in Coronado, one 40-minute session a week. The course was offered during regular class hours, at varying times so the same classes would not be repeatedly affected. “We had the best time. It was a blast.” She had 15 kids, mostly in fourth and fifth grade. Some took the materials home. One little girl was in complete denial about her asthma and wouldn’t even take the handout materials home, but most were much more actively involved. Six of the 15 parents attended the graduation ceremony, all said they had learned something.
With children as with adults, the challenge is to change the paradigm, to stop people thinking of medicine as a response to a crisis and to start thinking of prevention. (Time after time I hear asthmatics say that they’ve been on the inhaled steroids — the preventive medication — for a few weeks now, and they’re feeling so much better that they’ve started to cut down on all the drugs they’re taking. The first ones to go, of course, are the preventives, and the whole cycle starts back up again.) It’s very, very hard to convince someone, adult or child, to take a preventive, maintenance medication, Lynn Devine admits. She uses the sunscreen analogy. Mothers put sunscreen on their children before they go to the beach; think of asthma medication as sunscreen for the lungs.
Devine has visited about 40 schools, almost all elementary. There really isn’t a comparable program for junior high and high schools in San Diego. Of the 90 schools taking part in Open Airways this school year, 5 are junior highs, the rest elementary. “At that age they’re young enough to still take it from an adult. At high school they don’t want to hear it anymore,” Devine said. But that’s exactly the problem. At high school age, kids are least likely to behave wisely and in their own interests, even — especially, in some cases — if their lives are at stake. Peer pressure is at its strongest, and nobody wants to look like a geek. Every teenager wants to prove his independence, so who wants to be dependent on meds or be seen to be submissive to Mom’s worried nagging? Not to mention the fact that multiple hits from an albuterol inhaler will give you a buzz....
Open Airways is, in reality, only a start. According to Devine, “The program is finally acknowledging that there is a huge problem. The general attitude among teachers and the public at large is that asthma is as annoying as head lice and not much more dangerous. In the last couple of years 13 kids in L.A. have died from asthma. They don’t realize that even mild asthmatics can have a severe episode and die.”
The death of model Krissy Taylor seems to have been noticed by the high school community, thanks to her frequent appearances in Seventeen magazine. What may or may not have been picked up by teenagers is that she was using Primatene, an over-the-counter inhaler that is not recommended by doctors, or that asthma inhalers, which can give a buzz not unlike cigarettes, are the medication most frequently abused by dieters, after laxatives. People, in putting the unfortunate Taylor on their cover after her death, may have had as much effect as a hundred Open Airways programs. Or not. We’ll never know.
ANOTHER OPPORTUNITY FOR EDUCATION is the annual asthma camp, called Scamp Camp, after the Southern California Asthma Medical Program. This weeklong American Lung Association camp is held annually at Camp Marston, a YMCA camp at Julian, for roughly a hundred kids aged 8 to 13. Four daily medication sessions before meals and before bedtime are used to make medication normal, habitual. The kids also spend a little time learning about asthma. One of the most popular activities is the pigs’ lungs demonstration. Mike Welch brings in a compressor and pigs’ lungs so the children can start to visualize what is going on inside them, inflating and deflating the lungs, explaining lobes, bronchi, trachea. “They think it’s wonderful,” said Janet Wilson, who has volunteered at Scamp Camp. “It’s very gross, and kids just love gross stuff.”
The aim is also simply to provide a camp for kids with asthma. In many cases, these are kids who have never been allowed to go to camp for fear they would have an attack or receive inadequate supervision or simply not be able to take part in many of the activities. Some of the parents, then, see the asthma camp as a chance for their children to learn about asthma; for other parents it’s simply a chance to get the kids out of the house — a common enough motive for camp, but one that in this case might have the extra dimension of respite for the family. Having a severely asthmatic child is very demanding on the entire family. “For some of (the parents},” Wilson said, unaware of the loaded phrase she was using, “it’s the first breath of fresh air they’ve had.” The asthma metaphor works on both sides. In a sense, the entire family is suffocating.
ASTHMA DEMANDS A RADICAL CHANGE DI THE WAY SCHOOLS care for their kids. For example, asthma is all too often a furtive, almost invisible disease. The most dangerous situation is the kid who is using his inhaler every 20 minutes, wiring his metabolism from the medication but doing less and less good. Who sees this? If the kid is moving from room to room and class to class and doesn’t report his condition to the nurse, who knows? And this is exactly the profile for the worst-case outcome, the chronic but manageable condition creeping through the gray into the red zone without anyone around realizing how bad this could get. Then the collapse, the dash to the ER.
How do you monitor such a child? How do you make sure that good, regular prevention takes place, that he takes his meds as and when he should? Lynn Devine’s prescription: kids with moderate to severe asthma should have their medications in the classroom with them, but held by a teacher so that someone in a responsible position knows if the situation is starting to look dicey. (“Teachers will hate this,” she said, knowing full well how the coach is going to feel about having to sign in and carry eight inhalers in his bag to remember to give back at the end of class while everyone is off to the showers.) And those with severe asthma? Well, all severe asthmatics are recommended to carry a syringe full of epinephrine with them at all times. I can just imagine the principal’s face. A syringe?
What she is asking for involves a political change of the hardest sort. She wants the child to have the power to be able to say to an adult, “When I say I’m not feeling good, you have to listen to me.” By all accounts, this is especially hard where that power relationship is most overt — that is, in phys ed, especially in junior high schools and high schools. The coaches are seen as the dinosaurs here, the last perpetrators of the suck-it-up attitude. It’s not that the coach doesn’t understand asthma, it’s that he is more used to believing in authority. After all, isn’t physical education about the perfecting of the body so we don’t have to worry about it, he thinks, remembering the good old days when he could just tell them, “No pain, no gain,” or “Just do it,” and they’d blink and swallow and say, “Okay, Coach”? And thank him in the end, dammit.
Open Airways is good news, and I wish Devine and her colleagues every success. But the fact that things are going well in elementary schools shows our weaknesses and failings elsewhere. First, I tend to agree with Devine when she attributes her success to the fact that she isn’t a physician or a nurse but is driven by the passion and urgency of someone who has had a severely asthmatic child. She is, perhaps, not an expert in asthma but an expert in asthmatics. It is very rare to come across someone with medical training who recognizes how serious and frightening asthma is. When they call it a disease of neglect, they tend to overlook their own role in that neglect.
Second, the Open Airways program reflects the bizarre American attitude that we can and should care for children in precisely the areas that we cannot and should not care for adults. (The current V-chip television debate shows the same odd beliefs — that we have no right to control the content of television in the name of the general public, but we have every right and obligation to do so in the name of our children.) Asthma is just one of the diseases that flourishes in the absence of any semblance of a coherent and thoughtful social welfare system. Sickness is one of America’s punishments for being poor. Children, however, are seen as deserving better; but even so, it is worth noting that Open Airways is carried out voluntarily and by a nonprofit agency. Despite the Airwatch and advances in soluble inhaled steroids, America’s general care for Americans is still locked in the 19th Century.
Third, it’s also significant that Open Airways is being carried out in the schools. One result of this strange contrast between libertarianism for adults and protectionism for children is that schools are and will continue to be increasingly laden with the burden of fixing the ills (and illnesses) of society at large. (Hence the paradox of my daughter being taught in third grade that pollution is wrong on the same day the states were allowed to raise or even abolish speed limits.) And the younger the children, the more this is and will continue to be true. Open Airways doesn’t even try to address the issues at high school, where things are in some respects most difficult.
No matter how well-designed and well-delivered the program's message is, it comes down to 11-year-olds being given one message for six weeks. Who will carry on that torch? Who will maintain the consistency of that message in the face of Joe Charnel and a thousand other dangerous seductions?
IN SCKIPPS CLINIC, WHERE SOME GROUNDBREAKING RESEARCH into asthma and allergies has been taking place, I find myself sitting in on a lunchtime presentation by a drug company rep. His company has collaborated with the National Jewish Center for Immunology and Respiratory Medicine in Denver, arguably the top asthma center in the country, to produce a series of asthma education presentations, complete with four-color transparencies and slick handouts. While a dozen or so doctors and nurses eat gourmet pizza, he runs through his rap to solicit constructive criticism, partly because he wants to make sure his materials are accurate and useful, partly because he is hoping that Scripps will sign off on his project, allowing him access to the clinic’s patients.
The presentation is familiar stuff, pitched to an educated, middle-class, suburban audience, delivered in a jokey style. The Scripps people interrupt with corrections and questions. At one point the rep says, "Above all, I want to make Scripps Clinic happy.” Surely you mean Scripps Clinic’s patients, someone interjected. Of course, he said. Of course.
Did anyone see any ethical problem with a drug company employee making a direct representation to the public? “No,” three or four voices said immediately. Scripps had made sure that the drug company’s name would not appear on any of the presentation materials. Besides which, the rep added heatedly, promoting his own wares would be not only unethical but stupid. If there was one thing he didn’t want to do, he said, it was to get Scripps Clinic mad at him. “Several of my best clients are in this room.”
This cuts both ways. By erasing this professional affiliation, he is less clearly promoting his particular employer, but by the same token he is in effect, if not in name, presenting himself less as a drug company rep and more as a health educator, even a member of the medical profession.
In a sense, these objections are moot. Unless he knows something that Mary Beth Parr and Lynn Devine don't, he simply won’t have an audience, and the ethical question of drug companies pitching straight to the public won’t matter. I just think it’s interesting that, by all accounts, doctors can’t afford the time or the money to spend an hour or more with each patient, carrying out the education that may make the difference between gradual improvement and gradual decline; and insurance companies can’t afford to reimburse time spent on patient education, yet drug companies have enough free cash to research and develop their own education materials and pay someone to take them to the public.
THE BLEAKEST VANTAGE POINT FROM WHICH TO WATCH asthma — and to see all the cracks in what we flatteringly call a health-care system — is from the place where all the asthma failures end up: the emergency room.
Mary Margaret Loehr is a nurse in the emergency department at Scripps Memorial Hospital, Chula Vista. I had always assumed that once someone suffering from a life-threatening asthma attack reached the ER, the danger was more or less over. Wrong. She starts with inhaled beta-agonists, usually administered through a mask. In many cases the problem is the advanced inflammation, the airways swollen until they’re almost blocked, rampant with eosinophils and flaming with an internal biochemical warfare. This needs heavy doses of corticosteroids, either orally or through an IV, hut they won’t do much good for several hours.
If things look grim, she’ll administer a shot of epinephrine (adrenaline) or its cousin, terbutaline, which doesn’t have epi’s cardiac side effects. Some have to have the injection even if they have heart disease because otherwise they’ll die. The last resort is intubation — that is, literally sticking a tube down the throat into the lungs. This is such a traumatic procedure for someone who already can’t breathe that she’ll often have to paralyze and anaesthetize the patient.
“It’s a step to be taken with great trepidation. When you put them on a ventilator, your problems are just beginning. A severe asthmatic is very vulnerable to the increased pressure of the air being forced in and can easily blow out a lung.”
The classic asthma death is one with a slowly dawning sense of disaster. In fact, one of the common features is that the patient has no idea how compromised her breathing is, how bad things are getting. Typically, she is having some trouble breathing — nothing unusual there — and takes the inhaler every four hours, then every two as the relief gets shallower and shorter, then finally every 15 minutes. At some point, she realizes the inhaler is doing no good anymore and is having an increasingly toxic effect on her system. Her head is buzzing, she can’t think clearly. By the time she gets to the E.R, she has large clumps of thick mucus that can’t be dissolved, her airways are so swollen they' are clamped shut, and she dies.
Loehr is disturbed by a series of recent deaths that don’t fit this profile. What she and the paramedics have been seeing more often is a different scenario, one that should be extremely rare. At noon a young woman is walking with friends, apparently well; she says, “I don’t feel so good. I’d better use my inhaler.” Within minutes this becomes, “You’d better call 911,” and she is at death’s door with a terrifying suddenness. Whether this is just a statistical blip or not it’s hard to say, but combining her own experience with those of the local paramedics, Loehr said, “We’ve had a number of stories that were very clear cut. We’ve had several of those just in our own hospital.”
She suspects that familiarity has bred a dangerous contempt, or at least complacency — or maybe it’s the beta-agonist inhaler that has done so, making people think that asthma is trivial, that a single puff will take care of it. And it’s true that the vast majority of asthmatics, like diabetics, can lead normal active lives. But that very normality is deceiving. The paramedics see it all the time, she said. Johnnie takes his Cromolyn, runs with the soccer team, does fine. Coach is happy, Johnnie is happy that this asthma is no big deal, doesn’t keep him off the team, doesn’t make him look like a geek to his girlfriend. Then a time comes when the Cromolyn doesn’t seem to be working, nor do a second and third dose; it never occurs to him that this is a different beast. Asthma is a moving target.
Loehr also sees the patients who never appear in the suburban specialist’s office, whose only point of contact with modern American medicine, in fact, is the dash to the ER. In most cases, these are the very poor; and the very poor are far more likely to suffer from asthma.
The rise in the incidence of severe asthma in the U.S., which can be charted from the late 1970s, accompanies the steadily growing disparity between the increasing wealth of the wealthiest Americans and the increasing number of Americans who find themselves below the federal poverty standard.
Even more striking is the parallel between the rise in asthma among women and the feminization of poverty. Between 1979 and 1988, nearly a million families headed by women fell into poverty, until nearly half of the families headed by women were officially poor, a figure that rises to three-quarters among African Americans. Over the same period, asthma rates among women jumped dramatically. In 1980 slightly more males than females had asthma — 32 as opposed to 30 per thousand, according to the Centers for Disease Control — but by 1990 45 women per thousand had the disease, as opposed to 40 men. Most alarmingly, the number of women dying of asthma jumped 54 percent during the 1980s, compared to a 23 percent rise for men.
Asthma is one of the presenting symptoms of poverty. The fact that the wealthy also wheeze tends to cloud the fact that asthma is, in fact, a class issue. Studies in New Zealand, Scotland, and Britain have found that asthma is worst among low-income and one-parent families. At one time, I joined a mobile medical unit to visit a shelter for homeless families in New York. During the day, a couple of dozen families came out to the medical van parked outside the shelter, and whatever the reason for their wanting treatment, we found asthma in every single family.
The asthma itself has a further economic impact, contributing to a downward spiral. A New Zealand study of 93 adults attending a hospital-based clinic serving “a socially disadvantaged urban population” found that “repeated hospital admissions and frequent asthma-related sick days contributed to employer discrimination, job dismissal, and lack of career advancement.” Thirty-two percent of those currently employed said that they had difficulty getting time off work to attend the asthma clinic. Of those not working, 8.3 percent had lost their jobs because of asthma.
In the U.S., of course, poverty is intimately associated with race, and the black-white gap, always wide, has been widening. In 1979, blacks were about twice as likely as whites to die of asthma; by 1987 they were three times as likely, with the rate among black women ris-ing twice as fast as that among whites. In 1987, asthma death rates in East Harlem were nearly ten times the national average.
Physicians have been aware of the possible connections between these figures, but doctors are not known for being politically radical, and most researchers spend as little time as possible studying the poor. The experts tend to be quoted as saying that “the mechanisms involved” — that is, why the poor should get asthma — “are not well understood.”
Asthma is only one of the many burdens of poverty, its wheeze almost a metaphor for someone struggling to get along with the weight of the world on her shoulders. Under these circumstances, it seems almost a condition of existence, and as such it’s hardly surprising that it is hardly noticed, let alone treated. What can you expect? Why hope for more?
This hopeless and desperate outlook is the breeding ground for all kinds of pathologies, not just asthma. Many of those Loehr sees, especially those she sees regularly, are people who don’t appreciate the need for regular health care and immunizations, or who recognize the need but simply have no means of getting to a doctor, or who have no money and don t realize that some clinics may offer free care, or are too proud, or who simply have a very disorganized approach to life so that making and keeping an appointment is too much for them to handle.
A patient came in who was drunk and had lost her inhaler. Rather than giving her a prescription, which would have been beyond her ability to get filled, Loehr gave her an inhaler. A day or two later she was back again, drunk again, having lost that inhaler too. “There’s no way to link that asthmatic up to routine care, which is what she needs.”
For someone like this (and, arguably, for everyone), the need is for home care. America’s near-complete lack of home care is partly the result of a public failure of commitment; but, Loehr pointed out, countries such as Norway and the UK, which offer medical care that includes routine home visits, have no ghettos, no gang warfare, fewer homeless, few areas where it is unsafe for a nurse to walk in the daytime. (Of course, this raises the question of whether the lack of home health care is the result or the partial cause of these problems.)
And what if a health-care worker could make a home visit and meet a family with five children, all of whom were inadequately clothed, sheltered, immunized, and nourished, as well as suffering from asthma? Where should the medical dollar go? And if, as may well be the case, the problem is compounded by the parents’ pathologies, the visiting nurse is stymied, Loehr explained. The U.S. also has no social mechanism for removing kids from parents who are drug or alcohol addicted. The child’s asthma becomes a symptom, an index of the dysfunction of both the family and of America’s puny attempts at social welfare.
IT IS COMMON — IT'S ALMOST A RULE, IN FACT — to end articles about medicine in one of two ways. Either the last paragraph or two speaks of new research being conducted in a university somewhere and holds out hope of a cure, or the entire tenor of the piece is alarmist, and we are left with the fear that the latest virus or re-emergent bacterium has only to catch a plane to reach us, and humankind is only a breath away from epidemic extinction.
Dr. Edward Golub, formerly a professor of biology and director of research in the pharmaceutical industry, is now president of the Pacific Center for Ethics and Applied Biology and a partner in a group currently developing an interactive program for medical education that may be offered through an on-line virtual university. Dr. Golub suggests a different way of looking at asthma and at medicine in general.
In fact, suggests Dr. Golub, who lives in Solana Beach, most of us have always been wrong about how scientific medicine works. The Salk paradigm, the one-pathogen, one-illness, one-set-of-symptoms, one-treatment, one-drug, one-cure, one-happy-family view, the linear understanding of medicine that he constantly refers to as “the magic-bullet view,” doesn’t work with asthma, and in fact doesn’t work for most illnesses. Medicine never was this simple, although the history of medicine is often told as if it were. The decisive advances were always more subtle, broader-reaching than one drug: the introduction of sewers, the fluoridation of public water. These advances were not good stories and made no heroes. They were unglamorous and rarely the work of a single noble-browed (or Nobel-browed) genius.
The general future of disease will not be the single epidemic horror-virus such as Ebola; it will be endemic rather than epidemic, complex and nonlinear rather than singular. Asthma is a perfect candidate for disease of the future, as are panic attacks, depression, migraine, cancer, AIDS, MS, and the other autoimmune diseases. All of them flourish not in bad drains or mosquito swamps but in the weedy cracks in our paradigms for disease and health, in the dark spaces in our means of delivering health care.
He expands on ideas that he has set out in his book The Limits of Medicine. “The paradigm we’ve been functioning under since, say, 1920 is that health is the absence of disease, and it’s achieved through magic bullets provided by the biomedical-industrial complex, that because we are scientists and physicians and caring people, we’ve taken on almost a civic duty of taking care of the health of the nation. Everybody believed that, and they believed that (a) because we bedazzled them with science and (b) because nobody paid for the product, there were always third-party payers.”
Our faith in the ability of scientific medicine — that is, the biomedical-industrial complex — to find cures for all diseases was bolstered by the fact that from roughly 1945 onwards, newspapers and magazines told us repeatedly that our understanding of this or that disease was advancing and a cure was just around the corner. Our doctors’ powers over life, death, and even non-medical social problems were meanwhile being trumpeted on the new medium of television. More than a hundred American TV series featured doctors as heroes, far more than any other profession. The hospital became the place to rush in search of a cure, and instead of being a humble profession, medicine became a heroic one — not to mention a far more lucrative one.
Between 1950 and 1970, doctors’salaries nearly quadrupled, rising at almost twice the rate of college teachers’. (Drug companies have also been one of the most consistently profitable sectors of the American economy.) The country doctor described by Chekhov and William Carlos Williams still existed, but in popular culture his place had been rudely usurped by Dr. Kildare, and the doctor was replacing the cowboy as the mythic hero in whom a public, bewildered and impressed by the magical advances in medical science, could place its trust.
“Because it was such an appealing and free way of looking at things,” Golub went on, “and because during the era of infectious diseases it really worked, the public overlooked the fact that it was, in fact, a very, very, very lucrative operation, that the complex made scads of money, scads of prestige. Now things are changing. The very success of the system has caused the nature of disease to change. With the introduction of antibiotics, with public health and increases in the standard of living, by 1945 infectious diseases were so far in decline that they were manageable. With that came a steady decrease in infant mortality and a consequent lengthening of the life span.
“As [infectious] disease changed to chronic disease, there are no more cures. We can ameliorate symptoms, but we don’t talk about ameliorating symptoms. We still talk about curing disease. If you look at the fundraising from any one of the disease groups, it always ends. The cure is not here yet....’ It would be unthinkable to go around raising money by saying, ‘There will be no cure, but we might be able to find ways of preventing symptoms.’”
The perfect illustration of that, I suggested, is the for-profit cancer hospitals, which depict individual success stories of people who are still alive five years later. That is presented as a cure, even though that specific word may not be used.
“You don’t even have to go there. You can go to a not-for-profit major medical center. You show up there with a brain tumor. You’ll be told, ‘We’ll take care of everything. We’ll make arrangements for you to meet the radiologist who’s going to zap you, with the oncologist who’s going to treat you with these very, very toxic drugs, with the surgeon who’s going to go in and take out as much...and listen, I saw a patient with a tumor that size who recovered.’ Now the fact is that a young doctor probably has not seen such a patient but has heard from other doctors that every once in a while somebody does [survive]. But these people have never bothered to think about actual outcomes. It’s part of their training, it’s part of the ethos that this is what we do; and what’s expected when you die is that your survivors give comfort to the doctor for losing. So there’s nobody who is innocent here. Patients want to hear it.
“We are seeing, now, the beginning of a paradigm shift. The public confidence that the complex used to be able to count on has eroded. The flip side of gullibility is distrust and litigiousness. It’s no accident that now more office visits are made to practitioners of alternative medicine than scientific medicine. Far more out-of-pocket money is spent on alternative medicine than on standard medicine. The same people, by and large, go to their standard doctor, their insurance company pays for it, they’re not satisfied, and they try aromatherapy.”
This is particularly true, I suggested, of a chronic disease like asthma.
“Sure. Science itself is showing us how complex chronic diseases are, and it will be a miracle if we find actual cures for any of them. The Human Genome Project is just a logical extension of looking for specific magic bullets. The public is slowly and now more rapidly becoming dissatisfied, and the paradigm shift that is already becoming evident is redefining health, not as the absence of disease but as the presence of wellness. It’s starting with the educated higher-income population. I don’t know how far down it will trickle, but it’s no accident that smoking is falling off among educated people. It’s no accident that there has been a 25 percent decrease in cardiovascular disease in the last ten years in the absence of any medical advances, but largely through changes in diet.
“With this change comes a whole new definition of medicine and a whole new role for the doc. The doc is not there to find a magic bullet to cure you. The whole system is going to have to be there to help prevent, to help you change lifestyle, to help augment changes that are made, and to ameliorate symptoms, to delay the onset of debilitating chronic disease.”
The word “doctor” will have to return to its roots. It originally meant “teacher.” The old aggressive metaphors of “fighting” disease need to be quietly phased out, too, given that winning will no longer be an option; perhaps “coaching” might be a better metaphor.
“There was a recent article in Nature/Medicine by some people at MIT. The assumptions behind all the enormous amount of spending, primarily by the NIH, but also by the pharmaceutical companies, is that if we do science we’ll learn two things. We’ll learn how the world works, and because of that we’ll learn how to control the world. That’s what every scientist is taught. What [the authors of the article] point out is that we have been astonishingly successful, beyond our wildest dreams, in the first part. We really know how the biological world works. Not completely, but if you had told me when I started out in graduate school that we’d be cloning and sequencing genes, I would have said you’re nuts.
“And we’ve assumed that if we know how things work, the corollary would also be true, and we’d be able to control things. [The authors] point out that between 1935 and 1946 this really did work. If you look at the number of diseases for which an understanding gave you a treatment, it was astonishing. But if you look from 1946 on, there are few. Very few. And in fact there are new diseases which we can’t deal with. So even with all this enormous increase [in knowledge] the second part is not working, and maybe we have to start rethinking the premise.
“Now, that would be hard enough for the medical-industrial complex to do. It would be virtually impossible for the public. How are you going to tell them cancer is not going to be cured? We may delay it, we may prevent it, but it is not going to be cured. There may be no magic bullet for asthma.”
It’s true. How can one stop the runaway train of our belief in science to find a cure? Perhaps the asthmatic, then, especially the young asthmatic, is at the cutting edge in a change in all our perceptions, a new modesty of expectations. It is often said of childhood asthmatics that they display unusual maturity, a rare understanding of their abilities and their limits. Perhaps there can be nothing better and saner than to have a chronic but manageable disease, whose best and only treatment is to develop self-knowledge — that is, to understand oneself and one’s illness well enough to manage it successfully, to go beyond the frantic chase after illusory cures. Perhaps life itself involves such restrictions and flourishes within such limits.
Why Is Asthma on the Increase?
Some doctors argue that it isn't; it is simpty being better and more frequently diagnosed. The balance of opinion, though, is that more asthma is being diagnosed and more asthma is happening out there, especially severe asthma.
The temptation is to look for one cause, but asthma rejects such simplistic thinking. There are probably dozens of reasons, some overlapping, some nudging each other into action. For example:
Day Care. The number of children in day care has risen dramatically in the last 30 years. Perhaps a third of American three-to four-year-olds attend day care or preschool (in other countries, such as France, the percentage is even higher) where respiratory infections, the most common harbingers of pediatric asthma, run rampant.
Cats. In the last half-century, America’s affections have switched from dogs to cats, and the barnyard mouser has come indoors. Cat allergens (flakes of dead skin and hair) can linger in carpets and furniture for up to 24 weeks after the cat has been removed. Cat dander is such a powerful and easily transmitted allergen that it travels on people's clothes in astonishing quantities. A study in Sweden found higher levels of cat allergen in school classrooms than in some homes with cats, and recent research has even found high levels of cat dander in model homes in which no one has ever lived.
Dust Mites. In a curious way, dust mites suggest a weird link between asthma and comfort. For example, in a group of villages in Papua New Guinea, the incidence of asthma has risen from virtually nothing to more than 7 percent (in other words. Western levels) in the last quarter-century. Researchers discovered that over this period the New Guineans, who once had slept on bare earth floors, had acquired blankets, and the blankets were the first soft materials in these Spartan villages where dust mites could live and breed. Dust mites also flourish thanks to other modem conveniences:
Central heating. Modem climate control indoors ensures that dust mites and some molds can now have a year-round growing season.
Laundry detergents. Fifty years ago. everyone washed clothes and linens in hot water, which killed the thousands of dust mites inhabiting them. Now that we have developed cold-water detergents, the mites remain uncooked and emerge unaffected by water or soap.
Wall-to-wall carpeting. Once the preserve of the rich, it’s now a common feature of tract homes. The more the carpet, the more the mites.
Smoking. The only growth sector in the domestic tobacco market in recent years has been young women in their late teens and early 20s — in other words, in their prime childbearing years. Smoking both during and after pregnancy correlates with a greater likelihood of the child developing allergies, asthma, and respiratory problems of all kinds. But smoking is unlikely to be a growth factor in San Diego, which, according to the American Lung Association, has a lower smoking rate than any other major U.S. city.
Tim Brookes is the author of a book on asthma. Catching My Breath. He teaches at the University of Vermont and is a correspondent for National Public Radio.
Comments