{kind=link}
Here's something you might be interested in.
Ask a Hipster — Advice you didn't know you needed
Big Screen — Movie commentary
Blurt — Music's inside track
Booze News — San Diego spirits
Classical Music — Immortal beauty
Classifieds — Free and easy
Close to Home — What it’s like on the street where you live
Cover Stories — Front-page features
Drinks All Around — Bartenders' drink recipes
Excerpts — Literary and spiritual excerpts
Feast! — Food & drink reviews
Feature Stories — Local news & stories
Fishing Report — What’s getting hooked from ship and shore
From the Archives — Spotlight on the past
Golden Dreams — Talk of the town
The Gonzo Report — Making the musical scene, or at least reporting from it
Letters — Our inbox
Movies@Home — Local movie buffs share favorites
Movie Reviews — Our critics' picks and pans
Musician Interviews — Up close with local artists
Neighborhood News from Stringers — Hyperlocal news
News Ticker — News & politics
Obermeyer — San Diego politics illustrated
Outdoors — Weekly changes in flora and fauna
Overheard in San Diego — Eavesdropping illustrated
Poetry — The old and the new
Reader Travel — Travel section built by travelers
Reading — The hunt for intellectuals
Roam-O-Rama — SoCal's best hiking/biking trails
San Diego Beer — Inside San Diego suds
SD on the QT — Almost factual news
Sheep and Goats — Places of worship
Special Issues — The best of
Street Style — San Diego streets have style
Surf Diego — Real stories from those braving the waves
Theater — On stage in San Diego this week
Tin Fork — Silver spoon alternative
Under the Radar — Matt Potter's undercover work
Unforgettable — Long-ago San Diego
Unreal Estate — San Diego's priciest pads
Your Week — Daily event picks
Why don't doctors want to take Medi-Cal patients?
This Is the paperwork for a single case
Dr. Ted Mazer: "If you have your door open in a specialty practice to Medi-Cal patients, you would be inundated with them, and everyone you see loses money for the practice."
It's difficult to find a San Diego physician willing to comment on his experience, but when doctors do talk, reactions are consistent. Providers see themselves caught in a three-way dilemma.
Dr. Stuart Cohen: "A standard office visit is $50. Private insurance reimbursements range from $32 up to a full $50. Medi-Cal pays $14."
“I can’t afford it,” says Dr. John Beck, an orthopedic surgeon, about Medi-Cal. “The payment from the State of California is so low that I lose money seeing these people. I’m an orthopedic surgeon, and orthopedics, as a rule, requires a lot of expense on the part of the physician. For example, cast materials, braces, x-rays. I have to pay for all of that. When I’m not reimbursed for that anywhere near what I spend on it, then I’m actually paying out of my pocket to take care of these people. I’m sorry, but that is not a valid system.”
"Medi-Cal is the highest amount of personnel costs to bill, and it’s one of the lowest paying and a high denial rate for who the heck knows why."
Beck, 51, lives in San Diego and has an office in Mission Valley. Recently he has stopped accepting new Medi-Cal patients and now sees only those he was previously treating.
“For an anterior cruciate ligament operation on the knee,” he explains, “[my] surgeon’s fee is normally about $3000. There’s an assistant necessary, and that’s 20 percent, $600. The last ACL I did under Medi-Cal, I believe I was paid under $600 for it. The assistant was disallowed. So out of a $3600 bill, I was paid under $600. My overhead expense level is 40 percent. Forty percent of $3000 is more than $600.”
Dr. David Kaufman is a 52-year-old psychiatrist with a practice in Rancho Bernardo. There is still a little of his native Boston in his voice. His small but comfortable office is in an office building that looks more like a Spanish villa.
Dr. Kaufman says he sees Medi-Cal patients only on occasional referrals from other physicians. “With Medi-Cal it’s really very simple,” he says. “Medi-Cal just really doesn’t pay enough money — to physicians generally, but I think it’s even worse in psychiatry — so that one would be able to pay their bills. They’re asking people who have had at least eight years of schooling and training after college to work for $39 an hour. That’s what they’re paying now, $39 per patient, which is pretty much an hour. I think my handyman makes more. For them to expect someone with eight years of training after college to work for that rate is — to me it’s insulting. So it’s just that simple.”
“Frankly speaking, if you have your door open in a specialty practice to Medi-Cal patients,” says ear, nose, and throat specialist Dr. Ted Mazer, “you would be inundated with them, and everyone you see loses money for the practice. So there is no way to make a successful practice on Medi-Cal. The reimbursement is so poor that it costs us more to perform most services than we get reimbursed.” From behind his desk in his modest College Area office that overlooks Interstate 8, 37-year-old Dr. Mazer speaks very rapidly but clearly. He has short brown hair and piercing eyes.
Flipping through his office log, he offers examples of his Medi-Cal reimbursements. “In this office we’ll see referrals frequently with kids with recurring tonsillitis, which is something simple That child comes in, we see them for an initial office visit, and generally our charges would be about $70, and we get reimbursed $46. That happens to be one of the better reimbursements we get from Medi-Cal. Here’s a tonsillectomy. Our charge was $550. To give you an idea, that includes the preoperative visit, the surgery and the postoperative care in the office. Any follow-up office visits are also included in that charge. [Medi-Cal’s] reimbursement was $161. Most payers in the open marketplace would allow any where from about $400 to $700 for that procedure. When I first started practice in ’88, we routinely got $500 to $550 for that from most payers, and we’re talking getting one quarter of that [from Medi-Cal today].”
Most affected by low reimbursements are doctors who specialize in primary care, such as family practitioners and pediatricians. Their money is made by seeing several patients through the course of the day as opposed to one or two patients for a more expensive surgical procedure. More patients mean more paperwork, staff, and office space. The fixed costs of running a practice, therefore, are higher for primary care physicians. In most cases, more than half of the charges for primary care go to paying overhead costs. This makes primary care physicians like pediatrician Dr. Stuart Cohen especially reluctant to take low-funded Medi-Cal patients.
Dr. Cohen is tall and dark complexioned, with bushy black hair and mustache. His nicely decorated offices are in the College Area. He says he does not see any Medi-Cal patients except those he’s already treated whose families have hit bad luck or lost jobs and had to depend on Medi-Cal coverage, or follow-up care for patients he has first treated in a hospital.
“What’s happened is that state budgets and other cutbacks have limited the reimbursement rates on Medi-Cal to the point where the average payment for a pediatric visit basically doesn’t even meet our costs. A standard office visit is $50. Private insurance reimbursements range from $32 up to a full $50. Medi-Cal pays $14. If we counted overhead expenses — nurses, a nice office here with a lot of medical information systems, we can’t make a living off of it.”
One local ophthalmologist, we’ll call him Dr. Z, also limits his Medi-Cal practice to referrals and existing patients. He says “Well, in ophthalmology, the standard, complete eye examination is about $100. I don’t even know [what Medi-Cal pays], because whenever I’ve looked at it, it’s just depressing, so I don’t. I think it’s maybe $40 or something like that. Or cataract surgery. The charge is $3000. Medi-Cal pays about $900 to $950. So they are paying about a third of what charges are.”
Most of the doctors interviewed find their Medi-Cal patients, as a group, harder to treat. They are more likely to fail to keep appointments, which, the doctors admit, might be a transportation problem; but the doctors also observe that they rarely call to cancel, Also, some doctors say that Medi-Cal patients don’t follow treatment plans for one reason or another. One family practitioner, Dr. Gary McFeeters, cites the difficulty of seeing Medi-Cal patients as the main reason he won’t see most of them.
Slumped in his chair behind his desk in a modest, almost Spartan Linda Vista office. Dr. McFeeters speaks his mind with a low voice and relaxed manner. “As a rule, they are the most demanding as a group of patients. They pay nothing for their services, and they expect everything. They are the group that’s most likely to complain about everything that is done, and therefore they’re the most likely group to sue you in the event of a question. They have no money, and they can find you and manipulate the situation to their advantage. I’m not talking about all of them. I’m just saying it seems like this. They sometimes look at it as a good way to make money, off the doctor’s malpractice insurance.”
Dr. McFeeters, 47, who grew up in L.A. and Ventura Counties, is tall and thick and parts his blond hair in the middle. He complains that Medi-Cal patients, besides being demanding, are not reliable for appointments. “They are the most likely group of patients to make an appointment and not show or make an appointment and show up an hour late and want you to still see them. You understand, other people do this too, but as a group [Medi-Cal patients] are the most likely to do that.
“You’ll schedule a surgery, and you’ll have a long time marked off to do that, and they just won’t show up and won’t call.”
Dr. Kaufman offers his viewpoint on the matter. “When you’re dealing with Medi-Cal, you’re dealing with people who tend to have more problems and be more disorganized, and that’s why they’re in the situation they’re in. So most Medi-Cal patients are more difficult to deal with. They have less inner resources. Usually it’s not a question of their money resources. In general, they are less organized, less functional people with fewer sources, outside of their doctors, of support systems. So they are more difficult to treat. To oversimplify it, you’re being asked to take less than you can survive on to treat the most difficult patients.”
Dr. Mike Busch is a urologist whose practice is in the College Area. The 62-year-old physician has trim brown hair, graying a bit at the temples, and wears square-framed glasses. Model boats and nautical paraphernalia fill his office. Even the wallpaper is a nautical theme. Dr. Busch doesn’t turn away patients because they are on Medi-Cal. “I feel I have an obligation to take care of patients regardless of their insurance, regardless of their ability to pay,” he says.
He does agree, however, that Medi-Cal patients tend to be harder to treat. “Very often Medi-Cal patients are what we call ‘noncompliant,’ ” he explains, “whereby they don’t follow instructions very well. A lot of them have alcohol or drug dependency problems, so they are not really that concerned about following doctor’s orders. Sometimes, you write a prescription for medicine, and it’s not filled because it may cost them something to get the prescription filled. So they are a little tougher to handle than the more typical patient.”
He adds this qualifier, “I would say the majority of Medi-Cal patients are very compliant, very grateful.”
La Jolla pediatrician Dr. Bill Hitchcock says he does see Medi-Cal patients “if it’s a patient I’ve already had who has come across hard financial times, it’s a young single mother, or if they are referred to me by a physician that I know.”
Dr. Hitchcock’s office in the Golden Triangle area is strewn with children’s toys and books. It looks more like a kindergarten classroom than a doctor’s office. He is 38, has a pleasant, round face, dark hair, and a soft speaking voice. He says of Medi-Cal patients, “I don’t want to stereotype, but at times they can be a little bit harder to treat. Just from a statistical point of view, you are going to tend to probably run into more single-parent families. I hope this doesn’t sound bad, but you may be dealing with a little bit less-educated population — and that’s not meant in a derogatory sense — so therefore, compliance and follow-up appointments might be missed a little bit more commonly. At the same time, I have some wonderful Medi-Cal families. But yeah, I think they can be a little bit more challenging.”
Dr. Harold Brown’s office is on Second Avenue in Escondido. He is a gastroenterologist, a specialist in disorders of the stomach, intestine, and liver. Dr. Brown also complains that Medi-Cal patients “frequently do not follow up on the treatment plan that you give them, either because they are unable to financially or because they aren’t motivated to do so.”
Dr. Robert Bennett is also a gastroenterologist. Like Dr. Busch, he does not turn away Medi-Cal patients. “I take all comers,” he says. He is 64, has a jolly face and brown hair thinning at the hairline. You can clearly hear his New York City childhood in his voice. His small office is across the street from Sharp Memorial and Children’s Hospitals.
From Dr. Bennett’s experience, no-shows are common among all non-paying patients. “There is a much higher no-show rate in the office [with Medi-Cal patients] than there is with non-Medi-Cal patients. It’s a common occurrence. I teach at the university and the V.A. It’s an interesting thing with patients who are not directly responsible financially for part of their payment. When I’m teaching over there, they frequently have a 50 percent no-show rate for their appointments.”
From his experience, Dr. Mazer finds the patients themselves only third on his list of problems with the Medi-Cal system. “The patients are generally more demanding because they have no financial responsibility. Unfortunately, I’d have to say that they are the highest rate of no-shows; they make appointments and they don’t come in, which causes additional loss of income,” he says. “But for the most part, the problem is that Medi-Cal reimbursement is way below the actual cost of rendering the service, and the hassle factor is tremendous.”
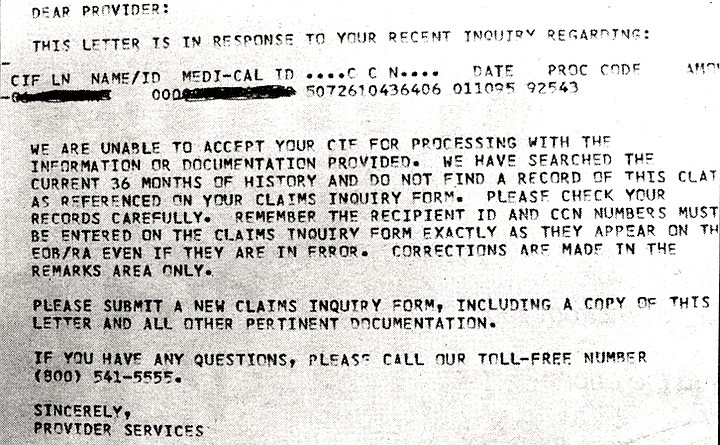
For Dr. Mazer and others who treat Medi-Cal patients, the hassle factor comes in the form of prior authorizations, complicated billing procedures, denials of payment, and overdue payments.
Dr. Davis Bronson, 47, is a plastic, reconstructive, and hand surgeon in La Mesa. He says he treats all Medi-Cal patients who come to him but also explains that he sees very few, because Medi-Cal doesn’t cover many types of plastic surgery. About the paperwork, Dr. Bronson says it’s burdensome. “It’s the inefficiency of it. The classic example is, you see a patient, and you want to request authorization to do an operation, so you send a special form in and it’s returned back to you [with authorization], You do the operation, and when you bill for the operation you send that form in with the bill, showing that you had authorization to do the surgery. Then your bill gets denied because [Medi-Cal claims] you did not have the form. Well, obviously it fell through the cracks somewhere. That happens quite frequently. In other words, the bureaucratic problems.”
Dr. Brown agrees, “Especially when you’re trying to get authorizations for procedures and medicines that you need to appropriately treat patients, requiring prior approval from governmental officials, and bureaucrats, and people who answer the phone to give you approval — who don’t even know what these procedures are, for the most part. You talk to someone who’s a phone-answerer, who doesn’t really know what they’re talking about They read out of a cookbook whether or not they should authorize.”
Asked how Medi-Cal paperwork compares with that of private insurance companies. Dr. McFeeters answers, “It’s worse in the fact that they’ll use any excuse to deny payment. You end up spending three or four months writing back and forth, time after time, to try to finally get reimbursed. For a $35 office visit, they’ll pay us — I can’t tell you the exact number — but they pay us $12 or $15. So by the time you add up the hours that it’s taken for your staff to prepare the letters, send the letters, and wait, and respond to their denials, we’ve probably spent way more than $35 to get the $12 to $15 they owed me in the first place.”
Medical-office manager Fern Wood says of the Medi-Cal billing process, “It’s just complete repetition. They return things for miscellaneous information, if there is something wrong on the identification. They also kick out things, stating that the patient is not eligible. Well, if the patient is not eligible, how come I received an eligibility okay [ from Medi-Cal] when I first saw that patient? It takes three months to get [the paperwork] correct because of all this bureaucratic crap. So these are really frustrating reasons why physicians don’t want to take any more Medi-Cal patients. We do take them on referral only.”
Ms. Wood says part of the frustration is dealing with what she calls Medi-Cal’s “five-dollar workers” responsible for accepting and authorizing claims. “I have a gentleman who is a student going to Grossmont College. He applied in December ’94 for Medi-Cal benefits. The request sat on the [Medi-Cal] worker’s desk for 45 days because she didn’t know what melanoma was. Melanoma is one of the deadliest cancers.”
Dr. Z credits such hassles as the main reasons he limits his Medi-Cal practice. “Medi-Cal has a completely different structure than any other insurance company, so the billing is completely different. They have their own handbook that is completely different, with all kinds of different numbers and different hoops to jump through in order to bill for Medi-Cal. And if you don’t follow that maze exactly, then they’ll deny it. And if you get something denied one time, you can almost forget it. Once it goes in, if you don’t do everything just perfectly right off the bat, it gets put in this ‘suspends,’ it’s kind of like limbo, and it just bounces around in that for who knows how long and who knows why. It’s a tremendous amount of work, office staff work. So it’s the highest amount of personnel costs to bill, and it’s one of the lowest paying and a high denial rate for who the heck knows why.
“I performed probably ten cataract surgeries that have been denied because they got into this denial thing; when you rebill it, it just goes away. That’s $10,000 that you do the work for, you do the right thing for the patient, and [payment is never made] because this maze of paperwork is not to their satisfaction — despite [physicians’] having consultants come in, despite going to courses on it, stuff gets messed up and you don’t know why. So you just end up writing off a surgery.”
And when Medi-Cal does pay, many doctors observe that payment is very late. Reading from his office log, Dr. Z says, “If I look at my accounts receivable over 120 days [past due], FHP is $500, Medicare is $1500, private insurance is $2400, railroad medical $1300. All of these are fairly low. Medi-Cal is $8369 over 120 days. So of all the insurances I take part in, M-C accounts receivable is five to eight times what it is for any other insurance.” He adds, “I think more physicians would be involved in Medi-Cal if it was simplified. [Doctors] would take a reduced rate if they could see the patient, do the work, get paid, and not have it be a hassle. But they don’t get paid very well, it’s such a hassle to do it, so they just walk away.”
In the past, as long as enough patients paid full price, doctors could afford to treat the nonpaying patients. As Dr. Bennett says, “I’ve been in practice 28 years. I’ve had people you can’t collect much on, but I’ve continued to do that. I’m able to do that because I have other people who pay better and can make up for some of it.”
However, some doctors consider this is no longer possible. The reason, they say, is that medical insurance companies, in particular health maintenance organizations (HMOs), have drastically reduced their reimbursements. Because most medical insurance comes through patients’ employers, and managed-care companies can offer them the best rates, the vast majority of medical care in the county is through managed care. In a nutshell, no one is paying full price anymore.
“Managed care has taken over San Diego,” declares Dr. Busch. “Sadly, the managed-care companies have discounted at least 30 percent of the normal fee for service; at least 50 percent would be more accurate.”
Dr. Mazer explains, “The more Medi-Cal patients you see in this practice, the more you have to make it up elsewhere; and, frankly speaking, there’s no place else anymore in the San Diego market to make it up. In the past, people saw a lot of indigent patients, and they would do it at no charge, and they' would accept the losses. Well, we still accept the losses; the problem is that in the past you could make it up on other payers, and you can’t do that anymore because of Medicare going down so low. We’ve lost at least 30 percent of our reimbursement in the last three years from Medicare. [Also,] the managed-care market has carved us down to rates at or below Medicare — in some cases, as low as Medi-Cal rates, and there are not a lot of patients left that aren’t on either a managed-care program or a government payer.”
Here's something you might be interested in.
Why don't doctors want to take Medi-Cal patients?
This Is the paperwork for a single case
Why don't doctors want to take Medi-Cal patients?
This Is the paperwork for a single case
Dr. Ted Mazer: "If you have your door open in a specialty practice to Medi-Cal patients, you would be inundated with them, and everyone you see loses money for the practice."
It's difficult to find a San Diego physician willing to comment on his experience, but when doctors do talk, reactions are consistent. Providers see themselves caught in a three-way dilemma.
Dr. Stuart Cohen: "A standard office visit is $50. Private insurance reimbursements range from $32 up to a full $50. Medi-Cal pays $14."
“I can’t afford it,” says Dr. John Beck, an orthopedic surgeon, about Medi-Cal. “The payment from the State of California is so low that I lose money seeing these people. I’m an orthopedic surgeon, and orthopedics, as a rule, requires a lot of expense on the part of the physician. For example, cast materials, braces, x-rays. I have to pay for all of that. When I’m not reimbursed for that anywhere near what I spend on it, then I’m actually paying out of my pocket to take care of these people. I’m sorry, but that is not a valid system.”
"Medi-Cal is the highest amount of personnel costs to bill, and it’s one of the lowest paying and a high denial rate for who the heck knows why."
Beck, 51, lives in San Diego and has an office in Mission Valley. Recently he has stopped accepting new Medi-Cal patients and now sees only those he was previously treating.
“For an anterior cruciate ligament operation on the knee,” he explains, “[my] surgeon’s fee is normally about $3000. There’s an assistant necessary, and that’s 20 percent, $600. The last ACL I did under Medi-Cal, I believe I was paid under $600 for it. The assistant was disallowed. So out of a $3600 bill, I was paid under $600. My overhead expense level is 40 percent. Forty percent of $3000 is more than $600.”
Dr. David Kaufman is a 52-year-old psychiatrist with a practice in Rancho Bernardo. There is still a little of his native Boston in his voice. His small but comfortable office is in an office building that looks more like a Spanish villa.
Dr. Kaufman says he sees Medi-Cal patients only on occasional referrals from other physicians. “With Medi-Cal it’s really very simple,” he says. “Medi-Cal just really doesn’t pay enough money — to physicians generally, but I think it’s even worse in psychiatry — so that one would be able to pay their bills. They’re asking people who have had at least eight years of schooling and training after college to work for $39 an hour. That’s what they’re paying now, $39 per patient, which is pretty much an hour. I think my handyman makes more. For them to expect someone with eight years of training after college to work for that rate is — to me it’s insulting. So it’s just that simple.”
“Frankly speaking, if you have your door open in a specialty practice to Medi-Cal patients,” says ear, nose, and throat specialist Dr. Ted Mazer, “you would be inundated with them, and everyone you see loses money for the practice. So there is no way to make a successful practice on Medi-Cal. The reimbursement is so poor that it costs us more to perform most services than we get reimbursed.” From behind his desk in his modest College Area office that overlooks Interstate 8, 37-year-old Dr. Mazer speaks very rapidly but clearly. He has short brown hair and piercing eyes.
Flipping through his office log, he offers examples of his Medi-Cal reimbursements. “In this office we’ll see referrals frequently with kids with recurring tonsillitis, which is something simple That child comes in, we see them for an initial office visit, and generally our charges would be about $70, and we get reimbursed $46. That happens to be one of the better reimbursements we get from Medi-Cal. Here’s a tonsillectomy. Our charge was $550. To give you an idea, that includes the preoperative visit, the surgery and the postoperative care in the office. Any follow-up office visits are also included in that charge. [Medi-Cal’s] reimbursement was $161. Most payers in the open marketplace would allow any where from about $400 to $700 for that procedure. When I first started practice in ’88, we routinely got $500 to $550 for that from most payers, and we’re talking getting one quarter of that [from Medi-Cal today].”
Most affected by low reimbursements are doctors who specialize in primary care, such as family practitioners and pediatricians. Their money is made by seeing several patients through the course of the day as opposed to one or two patients for a more expensive surgical procedure. More patients mean more paperwork, staff, and office space. The fixed costs of running a practice, therefore, are higher for primary care physicians. In most cases, more than half of the charges for primary care go to paying overhead costs. This makes primary care physicians like pediatrician Dr. Stuart Cohen especially reluctant to take low-funded Medi-Cal patients.
Dr. Cohen is tall and dark complexioned, with bushy black hair and mustache. His nicely decorated offices are in the College Area. He says he does not see any Medi-Cal patients except those he’s already treated whose families have hit bad luck or lost jobs and had to depend on Medi-Cal coverage, or follow-up care for patients he has first treated in a hospital.
“What’s happened is that state budgets and other cutbacks have limited the reimbursement rates on Medi-Cal to the point where the average payment for a pediatric visit basically doesn’t even meet our costs. A standard office visit is $50. Private insurance reimbursements range from $32 up to a full $50. Medi-Cal pays $14. If we counted overhead expenses — nurses, a nice office here with a lot of medical information systems, we can’t make a living off of it.”
One local ophthalmologist, we’ll call him Dr. Z, also limits his Medi-Cal practice to referrals and existing patients. He says “Well, in ophthalmology, the standard, complete eye examination is about $100. I don’t even know [what Medi-Cal pays], because whenever I’ve looked at it, it’s just depressing, so I don’t. I think it’s maybe $40 or something like that. Or cataract surgery. The charge is $3000. Medi-Cal pays about $900 to $950. So they are paying about a third of what charges are.”
Most of the doctors interviewed find their Medi-Cal patients, as a group, harder to treat. They are more likely to fail to keep appointments, which, the doctors admit, might be a transportation problem; but the doctors also observe that they rarely call to cancel, Also, some doctors say that Medi-Cal patients don’t follow treatment plans for one reason or another. One family practitioner, Dr. Gary McFeeters, cites the difficulty of seeing Medi-Cal patients as the main reason he won’t see most of them.
Slumped in his chair behind his desk in a modest, almost Spartan Linda Vista office. Dr. McFeeters speaks his mind with a low voice and relaxed manner. “As a rule, they are the most demanding as a group of patients. They pay nothing for their services, and they expect everything. They are the group that’s most likely to complain about everything that is done, and therefore they’re the most likely group to sue you in the event of a question. They have no money, and they can find you and manipulate the situation to their advantage. I’m not talking about all of them. I’m just saying it seems like this. They sometimes look at it as a good way to make money, off the doctor’s malpractice insurance.”
Dr. McFeeters, 47, who grew up in L.A. and Ventura Counties, is tall and thick and parts his blond hair in the middle. He complains that Medi-Cal patients, besides being demanding, are not reliable for appointments. “They are the most likely group of patients to make an appointment and not show or make an appointment and show up an hour late and want you to still see them. You understand, other people do this too, but as a group [Medi-Cal patients] are the most likely to do that.
“You’ll schedule a surgery, and you’ll have a long time marked off to do that, and they just won’t show up and won’t call.”
Dr. Kaufman offers his viewpoint on the matter. “When you’re dealing with Medi-Cal, you’re dealing with people who tend to have more problems and be more disorganized, and that’s why they’re in the situation they’re in. So most Medi-Cal patients are more difficult to deal with. They have less inner resources. Usually it’s not a question of their money resources. In general, they are less organized, less functional people with fewer sources, outside of their doctors, of support systems. So they are more difficult to treat. To oversimplify it, you’re being asked to take less than you can survive on to treat the most difficult patients.”
Dr. Mike Busch is a urologist whose practice is in the College Area. The 62-year-old physician has trim brown hair, graying a bit at the temples, and wears square-framed glasses. Model boats and nautical paraphernalia fill his office. Even the wallpaper is a nautical theme. Dr. Busch doesn’t turn away patients because they are on Medi-Cal. “I feel I have an obligation to take care of patients regardless of their insurance, regardless of their ability to pay,” he says.
He does agree, however, that Medi-Cal patients tend to be harder to treat. “Very often Medi-Cal patients are what we call ‘noncompliant,’ ” he explains, “whereby they don’t follow instructions very well. A lot of them have alcohol or drug dependency problems, so they are not really that concerned about following doctor’s orders. Sometimes, you write a prescription for medicine, and it’s not filled because it may cost them something to get the prescription filled. So they are a little tougher to handle than the more typical patient.”
He adds this qualifier, “I would say the majority of Medi-Cal patients are very compliant, very grateful.”
La Jolla pediatrician Dr. Bill Hitchcock says he does see Medi-Cal patients “if it’s a patient I’ve already had who has come across hard financial times, it’s a young single mother, or if they are referred to me by a physician that I know.”
Dr. Hitchcock’s office in the Golden Triangle area is strewn with children’s toys and books. It looks more like a kindergarten classroom than a doctor’s office. He is 38, has a pleasant, round face, dark hair, and a soft speaking voice. He says of Medi-Cal patients, “I don’t want to stereotype, but at times they can be a little bit harder to treat. Just from a statistical point of view, you are going to tend to probably run into more single-parent families. I hope this doesn’t sound bad, but you may be dealing with a little bit less-educated population — and that’s not meant in a derogatory sense — so therefore, compliance and follow-up appointments might be missed a little bit more commonly. At the same time, I have some wonderful Medi-Cal families. But yeah, I think they can be a little bit more challenging.”
Dr. Harold Brown’s office is on Second Avenue in Escondido. He is a gastroenterologist, a specialist in disorders of the stomach, intestine, and liver. Dr. Brown also complains that Medi-Cal patients “frequently do not follow up on the treatment plan that you give them, either because they are unable to financially or because they aren’t motivated to do so.”
Dr. Robert Bennett is also a gastroenterologist. Like Dr. Busch, he does not turn away Medi-Cal patients. “I take all comers,” he says. He is 64, has a jolly face and brown hair thinning at the hairline. You can clearly hear his New York City childhood in his voice. His small office is across the street from Sharp Memorial and Children’s Hospitals.
From Dr. Bennett’s experience, no-shows are common among all non-paying patients. “There is a much higher no-show rate in the office [with Medi-Cal patients] than there is with non-Medi-Cal patients. It’s a common occurrence. I teach at the university and the V.A. It’s an interesting thing with patients who are not directly responsible financially for part of their payment. When I’m teaching over there, they frequently have a 50 percent no-show rate for their appointments.”
From his experience, Dr. Mazer finds the patients themselves only third on his list of problems with the Medi-Cal system. “The patients are generally more demanding because they have no financial responsibility. Unfortunately, I’d have to say that they are the highest rate of no-shows; they make appointments and they don’t come in, which causes additional loss of income,” he says. “But for the most part, the problem is that Medi-Cal reimbursement is way below the actual cost of rendering the service, and the hassle factor is tremendous.”
For Dr. Mazer and others who treat Medi-Cal patients, the hassle factor comes in the form of prior authorizations, complicated billing procedures, denials of payment, and overdue payments.
Dr. Davis Bronson, 47, is a plastic, reconstructive, and hand surgeon in La Mesa. He says he treats all Medi-Cal patients who come to him but also explains that he sees very few, because Medi-Cal doesn’t cover many types of plastic surgery. About the paperwork, Dr. Bronson says it’s burdensome. “It’s the inefficiency of it. The classic example is, you see a patient, and you want to request authorization to do an operation, so you send a special form in and it’s returned back to you [with authorization], You do the operation, and when you bill for the operation you send that form in with the bill, showing that you had authorization to do the surgery. Then your bill gets denied because [Medi-Cal claims] you did not have the form. Well, obviously it fell through the cracks somewhere. That happens quite frequently. In other words, the bureaucratic problems.”
Dr. Brown agrees, “Especially when you’re trying to get authorizations for procedures and medicines that you need to appropriately treat patients, requiring prior approval from governmental officials, and bureaucrats, and people who answer the phone to give you approval — who don’t even know what these procedures are, for the most part. You talk to someone who’s a phone-answerer, who doesn’t really know what they’re talking about They read out of a cookbook whether or not they should authorize.”
Asked how Medi-Cal paperwork compares with that of private insurance companies. Dr. McFeeters answers, “It’s worse in the fact that they’ll use any excuse to deny payment. You end up spending three or four months writing back and forth, time after time, to try to finally get reimbursed. For a $35 office visit, they’ll pay us — I can’t tell you the exact number — but they pay us $12 or $15. So by the time you add up the hours that it’s taken for your staff to prepare the letters, send the letters, and wait, and respond to their denials, we’ve probably spent way more than $35 to get the $12 to $15 they owed me in the first place.”
Medical-office manager Fern Wood says of the Medi-Cal billing process, “It’s just complete repetition. They return things for miscellaneous information, if there is something wrong on the identification. They also kick out things, stating that the patient is not eligible. Well, if the patient is not eligible, how come I received an eligibility okay [ from Medi-Cal] when I first saw that patient? It takes three months to get [the paperwork] correct because of all this bureaucratic crap. So these are really frustrating reasons why physicians don’t want to take any more Medi-Cal patients. We do take them on referral only.”
Ms. Wood says part of the frustration is dealing with what she calls Medi-Cal’s “five-dollar workers” responsible for accepting and authorizing claims. “I have a gentleman who is a student going to Grossmont College. He applied in December ’94 for Medi-Cal benefits. The request sat on the [Medi-Cal] worker’s desk for 45 days because she didn’t know what melanoma was. Melanoma is one of the deadliest cancers.”
Dr. Z credits such hassles as the main reasons he limits his Medi-Cal practice. “Medi-Cal has a completely different structure than any other insurance company, so the billing is completely different. They have their own handbook that is completely different, with all kinds of different numbers and different hoops to jump through in order to bill for Medi-Cal. And if you don’t follow that maze exactly, then they’ll deny it. And if you get something denied one time, you can almost forget it. Once it goes in, if you don’t do everything just perfectly right off the bat, it gets put in this ‘suspends,’ it’s kind of like limbo, and it just bounces around in that for who knows how long and who knows why. It’s a tremendous amount of work, office staff work. So it’s the highest amount of personnel costs to bill, and it’s one of the lowest paying and a high denial rate for who the heck knows why.
“I performed probably ten cataract surgeries that have been denied because they got into this denial thing; when you rebill it, it just goes away. That’s $10,000 that you do the work for, you do the right thing for the patient, and [payment is never made] because this maze of paperwork is not to their satisfaction — despite [physicians’] having consultants come in, despite going to courses on it, stuff gets messed up and you don’t know why. So you just end up writing off a surgery.”
And when Medi-Cal does pay, many doctors observe that payment is very late. Reading from his office log, Dr. Z says, “If I look at my accounts receivable over 120 days [past due], FHP is $500, Medicare is $1500, private insurance is $2400, railroad medical $1300. All of these are fairly low. Medi-Cal is $8369 over 120 days. So of all the insurances I take part in, M-C accounts receivable is five to eight times what it is for any other insurance.” He adds, “I think more physicians would be involved in Medi-Cal if it was simplified. [Doctors] would take a reduced rate if they could see the patient, do the work, get paid, and not have it be a hassle. But they don’t get paid very well, it’s such a hassle to do it, so they just walk away.”
In the past, as long as enough patients paid full price, doctors could afford to treat the nonpaying patients. As Dr. Bennett says, “I’ve been in practice 28 years. I’ve had people you can’t collect much on, but I’ve continued to do that. I’m able to do that because I have other people who pay better and can make up for some of it.”
However, some doctors consider this is no longer possible. The reason, they say, is that medical insurance companies, in particular health maintenance organizations (HMOs), have drastically reduced their reimbursements. Because most medical insurance comes through patients’ employers, and managed-care companies can offer them the best rates, the vast majority of medical care in the county is through managed care. In a nutshell, no one is paying full price anymore.
“Managed care has taken over San Diego,” declares Dr. Busch. “Sadly, the managed-care companies have discounted at least 30 percent of the normal fee for service; at least 50 percent would be more accurate.”
Dr. Mazer explains, “The more Medi-Cal patients you see in this practice, the more you have to make it up elsewhere; and, frankly speaking, there’s no place else anymore in the San Diego market to make it up. In the past, people saw a lot of indigent patients, and they would do it at no charge, and they' would accept the losses. Well, we still accept the losses; the problem is that in the past you could make it up on other payers, and you can’t do that anymore because of Medicare going down so low. We’ve lost at least 30 percent of our reimbursement in the last three years from Medicare. [Also,] the managed-care market has carved us down to rates at or below Medicare — in some cases, as low as Medi-Cal rates, and there are not a lot of patients left that aren’t on either a managed-care program or a government payer.”
Comments