{kind=link}
Here's something you might be interested in.
Ask a Hipster — Advice you didn't know you needed
Big Screen — Movie commentary
Blurt — Music's inside track
Booze News — San Diego spirits
Classical Music — Immortal beauty
Classifieds — Free and easy
Close to Home — What it’s like on the street where you live
Cover Stories — Front-page features
Drinks All Around — Bartenders' drink recipes
Excerpts — Literary and spiritual excerpts
Feast! — Food & drink reviews
Feature Stories — Local news & stories
Fishing Report — What’s getting hooked from ship and shore
From the Archives — Spotlight on the past
Golden Dreams — Talk of the town
The Gonzo Report — Making the musical scene, or at least reporting from it
Letters — Our inbox
Movies@Home — Local movie buffs share favorites
Movie Reviews — Our critics' picks and pans
Musician Interviews — Up close with local artists
Neighborhood News from Stringers — Hyperlocal news
News Ticker — News & politics
Obermeyer — San Diego politics illustrated
Outdoors — Weekly changes in flora and fauna
Overheard in San Diego — Eavesdropping illustrated
Poetry — The old and the new
Reader Travel — Travel section built by travelers
Reading — The hunt for intellectuals
Roam-O-Rama — SoCal's best hiking/biking trails
San Diego Beer — Inside San Diego suds
SD on the QT — Almost factual news
Sheep and Goats — Places of worship
Special Issues — The best of
Street Style — San Diego streets have style
Surf Diego — Real stories from those braving the waves
Theater — On stage in San Diego this week
Tin Fork — Silver spoon alternative
Under the Radar — Matt Potter's undercover work
Unforgettable — Long-ago San Diego
Unreal Estate — San Diego's priciest pads
Your Week — Daily event picks
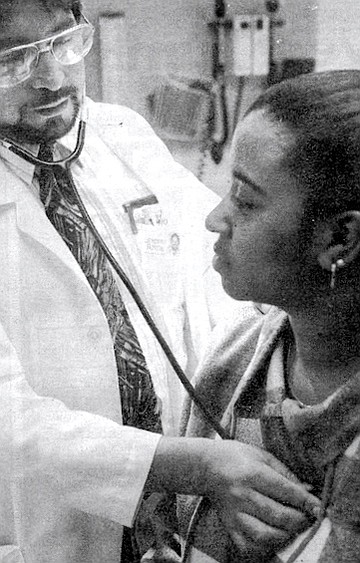
Medical intern training at Grossmont Hospital
"Did you push on her right upper quadrant?”

Jim Turnage: “If you’re going to get sick, don’t do it July 1. That’s the day the new year’s intake of interns starts."
Monday morning. Eight o’clock. Six doctors. Fourth floor. A small meeting room in Grossmont Hospital.
“What was the surgery finding?”
“Oh gosh! It was interesting. You reached in there, you felt that gallbladder — and it was crunchy. It was like crunch-crunch, crunch-crunch, wall to wall.”
Alberto Araya. It took until his late 30s before he could find the time to study medicine.
“That was your patient? The one who thought she was better?”
“Right. The one that wanted to leave.”
“And you know, the nurses, they just wanted to let her go. They said, ‘She’s not sick. She’s doing well. Let her go.’ I said, ‘No! I don’t want to let her go.’ The nurse said, ‘Well, I’m not going to get involved. I’m not going to get in between you and the patient.’ ”
“So she went into surgery?”
“Yes. This was at midnight, though....” Four residents (interns, apprentice doctors, most of them a year out of medical school) and two attending (supervising) physicians cluster around the table enthusing over the weekend’s admissions like kids rehashing a baseball game.

Fariba Ariz: “He refuses to eat. But there’s not much more we can do. He needs to go.”
Except here, accurate analysis counts. This is the meeting when each patient has to be accounted for. The interns must justify every medical decision they’ve made over the last 36 hours to the two attending doctors. This, in other words, is school.
“I really wanted to go to that surgery,” says Dr. Jim Turnage, a Dr. Kildaire-looking guy, complete with blond hair, blue eyes, white coat, and smiling face. He’s the only second-year resident.
“Everyone did!” says Dr. Fariba Ariz, a dark-eyed woman with black ringlets, gold ear studs, and a granny dress dotted with blue forget-me-nots. She’s one of the first-year residents.
“She’s a real interesting lady,” says Turnage. “Eighty-one years old. She came in with abdominal pains. At least, her husband said she had abdominal pain. She denied she had any. But in the work-up, it turned out she was a new diabetic, had pneumonia, had abnormal EKG — you couldn’t rule out myocardial infarction. She hadn’t seen a physician in over three years. So we had to look at everything. And one of these ‘everythings’ was this ultrasound....”
“That was a very good pickup, Jim. Did you push on her right upper quadrant?” asks Dr. Margaret Elizondo, one of the attending physicians, who looks vaguely like Linda Ronstadt.
“Alberto and I were just being obsessive-compulsive at the end of the day. It was, ‘Yes, you can go home to your daughter’s birthday party, and I’m going to go to sleep. And okay, one last thing.’ And we go by this [ultrasound] and whoa!”
“The compliment definitely goes to Jim,” says Dr. Venu Prabaker, the other of the two attending physicians.
“Oh, amazing pickup,” says Elizondo. “Very good. I was impressed.”
“Jim was persistent,” continues Prabaker. “He examined the patient. He could recognize that she was sick....”
“...Even though she had a normal white count, and no fever,” adds Elizondo.
“This is another classic case. The ideal case,” says Prabaker. “Absolutely no symptoms. And she wanted to go home! This is how geriatric patients can be.”
“It was Alberto who wouldn’t let her go home,” Turnage points out.
“She was pulling on the Foley bag [a urine-catcher],” says intern Dr. Alberto Araya. “I said, ‘Don’t pull! There’s a big balloon inside!’ She was trying to get it out. She was all dressed. She wanted to go home. ”
“That was amazing.”
“Great job, Alberto.”
“...So it was crunchy, huh?”
Everybody laughs.
The attention turns to Dr. Ariz. She starts reading from her weekend patient records.
“Mr. McDougal: He’s a 95-year-old man. Last time he saw a physician was five years ago. Basically he was sitting watching TV with his son. All of a sudden he had left-sided numbness, slurred speech, urinary incontinence, and confusion. No past medical experience except cataract surgery. Not taking any medication. Had a prostate operation back in 1985. Social history significant for drinking one beer and half a liter of wine a day. But he’s active. He walks about one and a half miles daily. His blood pressure was 208 over 132....”
She describes why she decided to admit the man, despite his 60-year-old son’s refusal to accept that his father could be sick. Prabaker and Elizondo seem to approve.
“The next one,” says Ariz, “is Jonathan Peters. This is a 30-year-old man with a history of seizures, hypertension...had a shotgun wound to his head because of a previous suicide attempt with a rifle, brought by paramedics to ER. He was found on a sidewalk, overdose....”
Ariz, Tumage, and the other interns at Grossmont Hospital aren’t doing the usual thing — learning how to become surgeons, pediatricians, or other specialists. They’re part of the charter year of an experiment to train medical graduates to become that old-fashioned Norman Rockwell hangover, the “family doctor.”
According to the program’s creator, Dr. Joseph Scherger, it’s nothing less than a medical revolution.
“In San Diego County, there’s one family physician for almost 4000 people,” says Scherger. “There really should be almost twice that many. And when you look at the family doctors that are in San Diego County, one-third of them are over the age of 60.
“In 1992, Sharp began looking at its resources — hospitals, various doctors, other services — and realized that one of the weaker areas of the health-care system was the number and quality of primary-care physicians — in particular, family physicians.”
Sharp must have seen which way the insurance wind was blowing. With costs rocketing and hospital bed rates plummeting, they needed to move medicine out of the hospital and back into the community.
That’s when Sharp decided it should “grow” its own family doctors. They called in Scherger, a pioneer in the family-practice revival. Dr. Scherger had been lecturing on the subject for 14 years at UC-Davis. He took two years to develop his program for Sharp and finally got it operating last July with the first six residents. He’ll expand this year to take in ten more neophytes and hopes Sharp will soon be at full capacity, training 20 future family practitioners a year.
But Scherger says the generation of doctors he’s creating is different from the old “country doc” figures. They’re actually becoming “wide-spectrum” specialists in their own right, better equipped than specialists to diagnose because of their “holistic” approach — from nutrition to preventive care to managing chronic problems to helping patients cope with anxiety and depression. And, as part of the hospital, the new doctors benefit from access to expensive machinery and the expertise of hospital specialists.
“The old-fashioned general practitioner,” explains Scherger, “would go straight from medical school to a rotating internship and then learn by experience. He wasn’t specifically trained to do modern, sophisticated primary care. The new residency-trained family physician is as much trained as a specialist as a surgeon is to do surgery.”
The impetus for changing the system, of course, comes from the insurance companies. “They’re the ones driving it,” says Scherger. “The new HMO or managed-care insurance plans require that a person choose a primary-care doctor. You aren’t free to take the four or five basic problems that you have and say, ‘Well, I want to go to four or five different specialists.’ Insurance companies aren’t willing to pay for that anymore, so they’re mandating this model. And what we’re doing is trying to provide doctors who can follow through with a more efficient, affordable model of health care.”
How big is the swing? “There have been 50 new family practice programs started nationally in the last 18 months, which is more than in the entire decade of the 1980s.” Scherger says 15 percent of medical students are now opting to become “Marcus Welby, MDs,” especially as stories proliferate in med school of specialists graduating, only to find themselves unemployed.
“We focus on the common problems of people,” says Dr. Scherger. “And that means a well-trained family doctor is equipped to handle between 85 and 95 percent of the reasons a person wants to see a doctor. When it comes to keeping people well and treating common health problems, that’s what we specialize in, and that’s what we train for.”
The GP, in other words, is back.
Only this time he’s not the independent shaman with a shingle on his shack. This generation is corporate, with umbilical cords firmly attached to various HMOs. The HMO GP. Standing, by HMO order, between you and the specialist of your choice.
To get his program going, Scherger has set up a family practice clinic right on hospital grounds. That’s where his interns spend half their time.
But the other half, the grueling half, Scherger has them sweating it out in the ER, the psych ward, the geriatric ward, the gyno ward — doing 36-hour stints every three or four days; keeping good, old-fashioned interns’ schedules, the kind that hospitals such as Mercy have long since abandoned as too tough for young docs.
9:00 a.m. Back at the caseload conference. Dr. Marie Shieh, a 29-year-old Chinese-American first-year resident, is outlining her weekend’s most spectacular patient.
“Joan Clayton,” she says. “Her chief complaint is she can’t breathe because of asthma. She’s 21, has had asthma since she was a child. Her mom has cats, dogs, birds, and horses, and she thinks she’s allergic to them. In January she was in a Nevada hospital for infected arthritis of her left ankle. Also had an episode of bronchitis-pneumonia in February. Also has gastric ulcers. She had a suicide attempt in ’93 — took a bunch of theophylline. Surgically, she had 32 teeth removed; she was born with two sets of teeth....”
Heads are shaking.
“I know, it’s amazing isn’t it? She’s also depressed, I don’t know exactly why, but she’s seeing a therapist and she has a psychiatrist. She is currently unemployed. Smoking: When she went to Nevada she started smoking, but she quit. Alcohol: Once in a while. She had three drinks this weekend with her mom. Drugs: She said she just tried pot and crystal but she doesn’t take drugs now. Family: Her dad has asthma and emphysema. The parents did smoke when she was younger, but nobody smokes at home anymore. She said she has had some rectal bleeding. She thinks it’s from her hemorrhoids.”
Dr. Shieh takes a breath. There’s more. “She’s been gaining weight since she was 19 years old, has had a sinus headache for the last couple of weeks, chest pain, and when I got down [to ER] she kept asking for more pain medicine. Vomiting, constipation, diarrhea, burning when urinating, yeast infection. Her skin was warm and moist, she had significant tenderness of her facial area, maxillary and frontal sinuses. Her throat was slightly red, cobblestoned, very little airflow through the lungs. Her sodium was 142, her potassium was 2.9, her white count was 11,400. Her chest x-ray showed scarring in the right middle lobe. She wanted an HIV test....”
She looks up.
“...I’m not really sure what to do with her.”
“I’d send her to Nevada, away from those pets. But then, she smokes there,” jokes Dr. Prabaker. Then he gets serious. “One of the things is education. She cannot go visit her mom, that’s for sure. The pets. Her mom can visit her, but only after a shower or something. It’s those clothes....”
“I told her to wash the cats weekly,” Shieh says. “That might help, but...”
“But just remember,” says Prabaker in his slightly sing-song Indian accent. “When you cannot breathe it’s extremely anxiety-producing. Hold your breath underwater, or just hold your breath! And in a minute what a horrible experience you’re getting, and anxiety causes more shortness of breath, and that causes more anxiety. It is a vicious cycle. You have to break that cycle by giving some Xanax.”
Prabaker hesitates. This man is said to be famous for his uncanny ability to diagnose, especially when symptoms aren’t clear. Nobody interrupts while he gathers his thoughts.
“One other comment. It’s important to realize that mortality is extremely high now among young bronchial asthma patients. It’s steadily increasing. We don’t know why. Some studies say 2 to 5 percent of patients can succumb. You have to be extremely careful.”
Dr. Shieh reads on through other admissions files, most of them clearly indigent — street people — until Dr. Prabaker finally pipes up for my benefit, perhaps embarrassed about the number of homeless people that make up Grossmont’s clientele.
“The patients who come to the hospital...we necessarily do a lot of [tests] on them just to save our skin. And it is an irony. The lawyers are making us do that. In no other country will we do that. We are wondering why the cost is going through the roof? This is one of the reasons.”
“Malpractice,” says Elizondo, shuffling her pile of three-by-five cards of the day’s patients. “The lawyers say, ‘Did you test for everything, absolutely every possibility? Rather than just the likelihood?’ ”
“And most of these patients,” says Prabaker, “come at the last moment, with decay or a very bad heart. They don’t take care of themselves. They come and get admitted, they want everything to be done, so we spend all kinds of money to do everything. Then before they recover completely, they go out, against medical advice, get out of the hospital for their next fix — only to come back two days later.”
Adds Dr. Turnage, “These patients typically have more complicated histories, with medical, psychiatric, and psychosocial problems. What we’re doing is expensive, and it’s very undercompensated.
“My regular patients,” continues Turnage, “don’t have to get a CAT scan every time they get a headache.”
10:00 a.m. Morning rounds. We’re coming down the fire-stairs to the third floor. Jim Turnage and Dr. Prabaker are doing their rounds together. “Marcus Welby, MD. That — truly! — is what I want to be,” says Turnage. He’s got a twinkle in his eye, but you can see he means it. “I’m not interested in being a specialist. People are the most important thing to me. Ever since I was a kid I’ve dreamed of being just this. The doctor in the white coat who looks after regular folks.”
We’re past the nurses’ station, into a room where an elderly woman is propped up on pillows, laboring at her breathing. “Hello, Mrs. Edwards,” Prabaker says. “How are we this morning?” “Congestive heart failure,” Turnage mutters, “asthma, emphysema, pneumonia, fluid in lungs. Exacerbated by diabetes. We use a vibrator to loosen up the sputum. There’s a lot of sputum.”
“You can go home soon,” says Prabaker. “But I very, very strongly recommend you make yourself a patient of Dr. Turnage, here.”
“I telephoned Social Security last week,” says Mrs. Edwards. “Talked to a nice lady, but I only get $452 per month....”
“Well, let’s ask our social services people to work on that, but I think you should continue to follow up with Dr. Turnage.”
“And I’m going blind,” says Mrs. Edwards, as though that might change Prabaker’s mind.
“Well, that’s why you need a regular doctor,” Prabaker tells her. “I’m offering Jim as Mrs. Edwards’s GP,” he says to me, “so he — and our other residents — can develop volume. Jim can take his patients with him when he completes here. I know how hard it can be starting out in private practice. When I began, I had to start from scratch. It was more difficult to gain the confidence and acceptance of patients, partly because I was different in appearance, but today I have a good reputation. And Jim — like 80 percent of doctors training here — he’ll stay in the area. The fact is, the good old family doctor is returning. Isn’t it, Mrs. Edwards?” Prabaker seems to be cheering Mrs. Edwards up. “I was born and raised here,” she says. “Used to work in a telephone answering service. Twenty years. I’ve probably talked to all three of you.”
We’re on our way to Room 311. “I’m not anti-specialist,” says Turnage. “But the U.S. has too many specialists.”
“And our wider perspective is needed,” says Prabaker, nodding constantly to nurses as we walk down the passageway. “Let me give you an example: A young girl, 16 or 17, came into my office with a fever. Rashes on the face. Tenderness on the back. Knee swollen. Her mother said to me, ‘You just do the fever. I’m taking her to a dermatologist for the spots, a chiropractor for the back, an orthopedic for the knee....’ She had not told each of these specialists about the other problems. I said, ‘Let me take care of the patient. I’m not here to take care of the fever, the rash, the knee....’ Because I’m trying to put all these things together. I found her sedimentation rate was 120. Her ANA [antinuclear antibodies] was 128,000. I told the mother I thought her daughter had systemic lupus. Well, now she was fuming at the specialists. But I said, ‘You can’t blame them. Especially if you never told them about the other symptoms.’ But in these cases you need someone general, who has some skills in all the fields. This is why we have the whole trend toward primary care. Because we are far better qualified than a patient to decide if and when a specialist is required, and which one. And of course, that saves the patient money, too.”
Turnage interjects, “All my medical education has been from specialists, but their focus is different than mine. For me, when you divide up a patient into parts, and you just look at an organ system — the skin, or the bones, or the endocrine system, or the glands of the body, or whatever — you lose the patient. And you lose the picture.... You’re likely to miss things. So, for a general internist like Dr. Prabaker, one of his joys in life, and his great expertise, is to look at a whole patient.”
“It’s like the old zebra joke,” says Prabaker. “If it’s striped like a zebra, gallops like a zebra, it probably is a zebra. Common sense plays a big part as well as scientific method. Jim’s patient with the acute inflammation of the gallbladder. Her EKG was abnormal, but she didn’t present with classic gallbladder symptoms. And besides,, she had pulled out her IVs. She wanted to go home. The nurses said she was competent. And according to the law, you have to let patients go. Anyone could have thought it was just pneumonia. Jim had already been on duty 39 hours. He could have said to [Dr. Araya] the first-year intern, ‘You take care of it.’ But something — instinct and training — told them both she was really sick. They telephoned her family to have them convince her to stay. Jim ordered an ultrasound. The radiologist was so impressed he ordered a CAT scan. And there it became apparent. Her gallbladder was gangrenous. It was about to burst! That surgery saved her life. No doubt about it. I’m impressed, really, Jim. Because residents usually don’t have the clinical acumen. This man is one of the best residents I’ve had.”
Turnage tries to swallow his pleasure at the praise. “That’s the thing in this job,” he says. “You really are affecting lives. It’s why I love it. I love being here.”
“It’s also why this trend is good,” says Prabaker. “If you need surgery, we go into the operating room with you, to assist. That way we can evaluate the surgeon. The patient is so grateful that you’re there, and we can see the surgery and the results. If six months down the road there’s further abdominal pain, we are familiar with the situation inside. You see? A nice web. The patient and the doctors are not so isolated as before.”
11:30 a.m. Room 311. Mrs. Lucille Teeter, 84. Also nearly blind. But she’s in for obstruction of the small bowel. A ball of gas in her tummy shows the painful backup.
“I’ve been in ten days and not a bite to. eat and nothing to drink,” she complains. But it’s a joke. In fact, she’s being fed intravenously. Mrs. Teeter has the most beautiful smile. And her eyes, even though they see only shapes now, are blue and clear. What she has is a terrible problem. Five to six bands are stretched across her bowel passage, obstructing the flow of waste materials. “It all started from scar tissue I got in 1929,” she says, “when I had my appendix out.”
“This lady is wonderful. Tough! A true positive thinker,” says Prabaker. “A year ago she had bypass surgery, and she perked up so well that by the fourth day she was out! That shows what can happen with a good positive attitude.”
“Good genes,” says Mrs. Teeter. “And I’m used to trouble. I was born on Christmas Eve, 1909, on a farm in Missouri, in the middle of a blizzard.”
Everybody laughs, but Prabaker and Turnage are worried. Prabaker decides it is time to call in a specialist, a gastroenterologist. As we leave, Lucille Teeter asks Prabaker to stay behind a moment. She wants him to tell her the truth. Is she going to get better?
We haven’t been ten minutes out in the hallway, waiting for Prabaker, when a beeper sounds. A nurse comes out. “Mrs. Teeter,” she says quickly. “She’s coded.”
Suddenly the hallway is awash in nurses running, carrying boxes, doctors and orderlies wheeling gurneys, all toward 311. Relatives appear, looking pale.
“Code Blue,” says someone hurrying by. “ Life-threatening.”
1:30 p.m. “She’s alive,” says Turnage, coming into the hospital cafeteria. He’s got a burger and a salad on his tray. “We’re still not sure if it was a little heart attack or not. We’ve shifted her to the IC [intensive care] floor.”
Turnage has just come from a monthly lunchtime meeting where doctors get together with a facilitator and express personal frustrations with the job. A kind of encounter group for those always coping with other people’s problems.
“There’s a very definite pecking order,” says Turnage, the senior man among the interns.
“The chairman of the department, the senior residents, the junior residents. My job is to guide the junior guys.”
He brings out a little book. It looks like the equivalent to Mao’s little red book. Much thumbed. “This,” he says with mock awe, “is Chan. My bible. Current Clinical Strategies in Family Medicine. It has little mnemonics in it like...SOAP. When [a first-year resident] describes a patient to me, they should always do it in this order. Subjective: What the patient thinks is wrong with him/herself. Objective. What the doctor thinks is wrong. Assessment. His overall feeling as to the patient’s situation. And Plan: What he’s going to do about it. SOAP.”
He flicks to another page. “The other character we come to know well is ADCA VAN DIMSL. I ask what they’ve done about a patient, and they run through ADCA VAN DIMSL: Admit, Diagnosis, Condition, Allergies? Vital signs? Ambulation? Nursing? Diet? IV fluids? Medicines? Special circumstances — like diabetics — and Labs. We do it in that same order till it becomes automatic.”
For an intern, it turns out, Jim Turnage is no spring chicken. He’s 47. In fact, most of his adult life he’s been a Marine or a musician, playing clubs in San Francisco, L.A., and San Diego, even making a few records. He’s originally from Dallas, Texas.
“I’d wanted to be a doctor since I was a little kid. But I couldn’t imagine that I’d ever be good enough to do it. So basically I had to live a fairly long adult life to come to the realization that yes, I could do that.”
He graduated in 1965 from high school, went to Stanford in the “fabulous ’60s,” completed a degree in statistics there, and “in my own personal response to the Vietnam War,” joined the Marines as a flight officer. He was in the back seat of Phantom F-4s. “That catapult launching off carriers — it made me want to be an astronaut, to get that extra kick. It was a thrill in itself.”
When he got out in 1973, after four years in the Marine Corps, he went back to music. He was out there jammin’ all the way through ’86. He’s still a guitar-player and singer-songwriter, still has a little studio in his house.
So how did he make the leap from steel guitar to stethoscope?
“It sounds really mundane, but I analyze my life a couple of times a year — at my birthday in August and the calendar new year; a little brainstorming and prioritizing. One year on my birthday, I did my list, and once again the physician thing kept coming up to the top. So this time I acted. I went to a local college to ask about med school, and they said, ‘You won’t get in because you’re too old.’ I was 36 at that point, 1984.
“But I did it anyway. I went back to school, did all the pre-med courses in 11 months. At that point I was a little out of sync for getting in the application cycle. So I became a high school teacher for a year — in South Central Los Angeles. That was transforming. Locke High School was built right on the site where the Watts riots were in 1965. And it’s everything you’ve ever heard about. We were in Crips territory, lots of gangs, violence — but guess what? I learned something from those kids. If I hadn’t gotten into medical school, I would have stayed there. Every day was a net positive, because the kids somehow would come through, despite all their circumstances.
“Then I got accepted into medical school. A Jesuit school in St. Louis. There was a singular difference in the way it approached medicine. We spent a significant amount of time studying about the bio-psycho-social things that I’m interested in. Typical ’60s.”
Still, he almost went for surgery.
“I did surgery as my first rotation. And I loved it. I thought it was a fascinating, exhilarating experience. I got to assist on an amazing array of surgeries. These are things I will never get to do again in my life. Liver transplants, for instance.
“It seems a bit macabre to people who are not involved in the medical business, but to have your hand in someone’s belly, helping surgically correct something that will allow them to live or palliate their pain, it’s an...experience. Especially if you know the person. Your eyes, your hands, all your senses are involved. The honor to be able to do this. I was so blown away.
“I worry about people who are going through their lives doing things they don’t want to do. I feel really privileged that I’ve been able to do things that I want to do. I truly do this for fun.”
3:00 p.m. Turnage is busy in a cubicle with the Physicians’ Desk Reference. He’s signing someone out, a poor woman who got brain damage in a multi-car pileup. Turnage says she has “profound injuries” to the brain, her awareness of her environment is way down, her swallowing is shot, she tends to breathe down food, she’s subject to pneumonias. Her family has asked for no heroic measures. Her prognosis, Turnage says, is for a “stormy course.”
I wander over to Dr. Fariba Ariz, leaning over the nursing station counter, waiting for a patient’s records. A tall lady named Leslie comes up to her. She’s from the hospital’s social services. “Any luck with Mr. Jones?” Ariz asks her. “He refuses to eat. But there’s not much more we can do. He needs to go.”
“Nobody wants to take him,” says Leslie. She’s talking about board-and-care facilities where she sends patients to convalesce, so they don’t take up expensive hospital space — or end up back on the street, where they often die. “They all say they have no beds, but people like him, they don’t want to take them.” She shakes her head sadly. “It’s a dirty business.”
Mr. Jones, it turns out, is indigent. He has hepatitis C, “end-stage,” as Ariz puts it. A friend from the sheriff s department brought him into Grossmont’s ER.
“Well, keep trying,” says Ariz. She’s 27, looks younger. Yet she’s donning plastic gloves, plastic smock, and a face mask, on her way to see a man dying from an infectious liver disease.
Inside Room 237 you first notice blankets. All you can see of Mr. Jones is a long mass of beautiful brown chestnut hair spread over the pillow. Oprah is blurting out from a wall-mounted television.
“Mr. Jones? Are you cold? We’ll get you another blanket.”
Mr. Jones is sleeping. The exhausted sleep of a body under assault. Ariz leans over, gets Mr. Jones to turn slightly. He’s not an old man, maybe 40. But his face is deep yellow. He’s hardly responding. She touches his stomach. “Does that hurt?” He smiles, perhaps a wince of pain.
“This is not a well-oriented liver,” she mutters.
A few minutes later, outside again, she takes off the mask and gloves. “He’s dying,” she says. “Slowly. He has a very big liver, fluid over the stomach. He’s weak. He can’t eat. And nobody wants to take care of him. He doesn’t have insurance. If he did [the board-and-care facilities] would accept him in a minute. His enzyme levels are worse and worse. Next time he comes it’ll be...”
She doesn’t finish the sentence. This isn’t the first time she’s encountered death.
Back in 1979, 11-year-old Fariba Ariz got used to staring down at dead bodies in the rubble after Iraqi bombing raids. The Iran-Iraq war had come to Teheran.
“Every day we would hear the bombs. When bombing happened they would have airraid sirens that would warn the whole town. But sometimes the planes would come even before the sirens. The first thing you’d hear would be a big shake — the whole ground. Then you’d just run down to the basement, the whole family, and you wait and wait.... Those nights, everything had to be done with candles. Your parents — you got to see them in a different time in their life. You had never seen them facing death before. We became very close. What I saw was not something a lot of people see. You basically see life and death. Any minute you can die.”
That possibility became personal too. Ariz’s father was a top oil executive. With the revolution, there was a worry that anti-Shah rebels would kidnap her because of her father’s position. “I was [put] in a military camp, living with another family, friends of my father, until he thought it was safe. Now when I look back, I’m just happy that I had that experience. Your view to life changes when you see the worst things that can happen. The little things don’t bother you anymore. Your views are a lot different.
“That’s actually what made me interested in becoming a physician. To be able to help my family, and people, wherever they are, in any situation.”
Despite that early experience, she says dealing with patients’ personal crises was hard, especially at first.
“There was a patient in the first month when I was an intern here, an elderly gentleman, and we found out he had leukemia, and he was in such bad condition that he was asking me, ‘Why can’t God take me away?’ That was very hard, to try to tell him to ‘have hope’ and ‘don’t give up,’ seeing him like that and wanting to die. But you learn. I try to use their strength. A patient who is dying, I’ll find out his worst worry, perhaps that his children are going to be without their father, so I try to find the children and bring them in so they can resolve that issue with him.”
Ariz likes the direction American medicine is taking. “In Iran, it’s family practice. Most people have a family physician for life. In the future I think it’s going to be more family physicians too. But it’s tough training to be a doctor here. We have to get loans — $80,000 to $100,000. And that’s without interest. You can imagine by the time you graduate how much interest has accumulated. I just think it’s not fair, realizing that all you do, 24 hours a day, almost, is care for patients, and the amount of money that you earn as a family physician is not enough to be able to pay these loans off right away. Our loan interests are not even tax-deductible. It’s very difficult. I had to take a lot out in loan money. I’ve just been talking to a loan company, trying to defer these loans. In other words, we are very poor doctors.”
Now she’s on her way to the farthest room on the floor. It’s old Mrs. Lassiter. “COPD,” says Ariz, quietly. “Chronic obstructive pulmonary disease. Emphysema. She’s depressed. Her family is not too keen to take her. When I go in she basically cries. She’s worse than discouraged.”
Inside the room, a little lady lies with tubes up her nostrils, breathing shallowly. Ariz puffs her pillows, has her lean forward and breathe as deeply as she can while she listens with her stethoscope on Mrs. Lassiter’s back. “Definitely better,” she says. “You are getting better, but slowly. So we need to be thinking about moving you somewhere where you can get better. A Transition Care Unit.”
“Oh no!” says Mrs. Lassiter, panicking. “I went to one once. They were rough and rude and crude. The nurses had no compassion. I don’t want to go to one of those places! I want to stay here.”
“If you stay here, we’ll have to send you home,” says Ariz. “We can’t do any more for you. You’re getting better. Truly.”
Tears are rolling down Mrs. Lassiter’s cheeks. Her strained breathing is fitful. “I don’t want to go today, because...I’m not ready! I don’t want to be pushed around again. Can’t I stay till tomorrow?”
“I think we have a deal here,” says Ariz. “You agree to the TCU — it’s just downstairs — and we’ll let you stay here tonight.”
Mrs. Lassiter takes a long breath. “Would you talk to my daughter?” she asks Ariz.
As the day wears on — and it is a long one, constantly on your feet, constantly talking with people in trouble — it becomes apparent that all the interns here are unusual people. Unusual in their outlook, unusual in the journey that brought them to this profession.
Alberto Araya, of crunchy gallbladder fame, is passing through on his way downstairs for 12 more hours in the ER. Araya, in his 40s, also came late to doctoring. He’s from Chile and has had a family to look after for 20 years. Like Jim Turnage, it took until his late 30s before he could find the time to study medicine.
Marie Shieh, on her way back from the psychiatric ward, says she became a doctor “to spite” her family, because they wanted her elder brother to take on the task. “But my father did always want me to have a career so I wouldn’t be dependent on a husband,” she says. “They were pleased when I graduated. They never expected it out of [their daughter]. Asian people push their children. They want their kids to be respected.”
Marie is married to an (Anglo-American) acupuncturist, whom she met while she was teaching for a year in provincial China. She wants to set up a dual clinic with her husband, offering medicine from “both worlds.” She “has a big social leaning” and believes in socialized medicine, such as the Canadian single-payer system. She thinks doctors are overpaid and would like to go work for the World Health Organization one day. Yes, the interning is hard work, she says, but “I just love to come in here to work. It’s like a drug. Only thing is, your spouse has to be extremely understanding.”
But the job carries its share of horrors and doubts. Shieh still tortures herself over a patient who “died on me” — an 83-year-old lady who came in with heart problems. “It was 5:00 in the morning. I was tired. She looked in good shape. We talked. She was alert, intelligent. I liked her. We did an electrocardiogram, and I suddenly realized her heart was a ticking time bomb. Half an hour later...she was dead. Aneurysm in the aorta. It had burst. I go over and over that morning, thinking, ‘If I’d been quicker....’ ”
5:00 p.m. As I walk out of the hospital and down to Grossmont Center, leaving all these personal dramas behind, I think of myself at Ariz and Shieh’s ages, late 20s, committed to — what? A good time? A general plundering of the world’s riches? Is it because this group of interns are minority Americans that they have stronger values of family and duty than I ever had?
It looks like this crowd of new doctors will give it back, in spades. And if they’re heralding an era when doctors are encouraged to be “people” people, as opposed to scientists looking for lab rats, that has to be a good backward-step-forward for American medicine.
But as I prepare to enter the world again, I remember Dr. Turnage’s last words:
“If you’re going to get sick, for God’s sake don’t do it July 1.”
I asked him why not.
“Because that’s the day the new year’s intake of interns starts,” he says. “Believe me, they’ll all be very nervous.”
Here's something you might be interested in.
Medical intern training at Grossmont Hospital
"Did you push on her right upper quadrant?”
Medical intern training at Grossmont Hospital
"Did you push on her right upper quadrant?”
Jim Turnage: “If you’re going to get sick, don’t do it July 1. That’s the day the new year’s intake of interns starts."
Monday morning. Eight o’clock. Six doctors. Fourth floor. A small meeting room in Grossmont Hospital.
“What was the surgery finding?”
“Oh gosh! It was interesting. You reached in there, you felt that gallbladder — and it was crunchy. It was like crunch-crunch, crunch-crunch, wall to wall.”
Alberto Araya. It took until his late 30s before he could find the time to study medicine.
“That was your patient? The one who thought she was better?”
“Right. The one that wanted to leave.”
“And you know, the nurses, they just wanted to let her go. They said, ‘She’s not sick. She’s doing well. Let her go.’ I said, ‘No! I don’t want to let her go.’ The nurse said, ‘Well, I’m not going to get involved. I’m not going to get in between you and the patient.’ ”
“So she went into surgery?”
“Yes. This was at midnight, though....” Four residents (interns, apprentice doctors, most of them a year out of medical school) and two attending (supervising) physicians cluster around the table enthusing over the weekend’s admissions like kids rehashing a baseball game.
Fariba Ariz: “He refuses to eat. But there’s not much more we can do. He needs to go.”
Except here, accurate analysis counts. This is the meeting when each patient has to be accounted for. The interns must justify every medical decision they’ve made over the last 36 hours to the two attending doctors. This, in other words, is school.
“I really wanted to go to that surgery,” says Dr. Jim Turnage, a Dr. Kildaire-looking guy, complete with blond hair, blue eyes, white coat, and smiling face. He’s the only second-year resident.
“Everyone did!” says Dr. Fariba Ariz, a dark-eyed woman with black ringlets, gold ear studs, and a granny dress dotted with blue forget-me-nots. She’s one of the first-year residents.
“She’s a real interesting lady,” says Turnage. “Eighty-one years old. She came in with abdominal pains. At least, her husband said she had abdominal pain. She denied she had any. But in the work-up, it turned out she was a new diabetic, had pneumonia, had abnormal EKG — you couldn’t rule out myocardial infarction. She hadn’t seen a physician in over three years. So we had to look at everything. And one of these ‘everythings’ was this ultrasound....”
“That was a very good pickup, Jim. Did you push on her right upper quadrant?” asks Dr. Margaret Elizondo, one of the attending physicians, who looks vaguely like Linda Ronstadt.
“Alberto and I were just being obsessive-compulsive at the end of the day. It was, ‘Yes, you can go home to your daughter’s birthday party, and I’m going to go to sleep. And okay, one last thing.’ And we go by this [ultrasound] and whoa!”
“The compliment definitely goes to Jim,” says Dr. Venu Prabaker, the other of the two attending physicians.
“Oh, amazing pickup,” says Elizondo. “Very good. I was impressed.”
“Jim was persistent,” continues Prabaker. “He examined the patient. He could recognize that she was sick....”
“...Even though she had a normal white count, and no fever,” adds Elizondo.
“This is another classic case. The ideal case,” says Prabaker. “Absolutely no symptoms. And she wanted to go home! This is how geriatric patients can be.”
“It was Alberto who wouldn’t let her go home,” Turnage points out.
“She was pulling on the Foley bag [a urine-catcher],” says intern Dr. Alberto Araya. “I said, ‘Don’t pull! There’s a big balloon inside!’ She was trying to get it out. She was all dressed. She wanted to go home. ”
“That was amazing.”
“Great job, Alberto.”
“...So it was crunchy, huh?”
Everybody laughs.
The attention turns to Dr. Ariz. She starts reading from her weekend patient records.
“Mr. McDougal: He’s a 95-year-old man. Last time he saw a physician was five years ago. Basically he was sitting watching TV with his son. All of a sudden he had left-sided numbness, slurred speech, urinary incontinence, and confusion. No past medical experience except cataract surgery. Not taking any medication. Had a prostate operation back in 1985. Social history significant for drinking one beer and half a liter of wine a day. But he’s active. He walks about one and a half miles daily. His blood pressure was 208 over 132....”
She describes why she decided to admit the man, despite his 60-year-old son’s refusal to accept that his father could be sick. Prabaker and Elizondo seem to approve.
“The next one,” says Ariz, “is Jonathan Peters. This is a 30-year-old man with a history of seizures, hypertension...had a shotgun wound to his head because of a previous suicide attempt with a rifle, brought by paramedics to ER. He was found on a sidewalk, overdose....”
Ariz, Tumage, and the other interns at Grossmont Hospital aren’t doing the usual thing — learning how to become surgeons, pediatricians, or other specialists. They’re part of the charter year of an experiment to train medical graduates to become that old-fashioned Norman Rockwell hangover, the “family doctor.”
According to the program’s creator, Dr. Joseph Scherger, it’s nothing less than a medical revolution.
“In San Diego County, there’s one family physician for almost 4000 people,” says Scherger. “There really should be almost twice that many. And when you look at the family doctors that are in San Diego County, one-third of them are over the age of 60.
“In 1992, Sharp began looking at its resources — hospitals, various doctors, other services — and realized that one of the weaker areas of the health-care system was the number and quality of primary-care physicians — in particular, family physicians.”
Sharp must have seen which way the insurance wind was blowing. With costs rocketing and hospital bed rates plummeting, they needed to move medicine out of the hospital and back into the community.
That’s when Sharp decided it should “grow” its own family doctors. They called in Scherger, a pioneer in the family-practice revival. Dr. Scherger had been lecturing on the subject for 14 years at UC-Davis. He took two years to develop his program for Sharp and finally got it operating last July with the first six residents. He’ll expand this year to take in ten more neophytes and hopes Sharp will soon be at full capacity, training 20 future family practitioners a year.
But Scherger says the generation of doctors he’s creating is different from the old “country doc” figures. They’re actually becoming “wide-spectrum” specialists in their own right, better equipped than specialists to diagnose because of their “holistic” approach — from nutrition to preventive care to managing chronic problems to helping patients cope with anxiety and depression. And, as part of the hospital, the new doctors benefit from access to expensive machinery and the expertise of hospital specialists.
“The old-fashioned general practitioner,” explains Scherger, “would go straight from medical school to a rotating internship and then learn by experience. He wasn’t specifically trained to do modern, sophisticated primary care. The new residency-trained family physician is as much trained as a specialist as a surgeon is to do surgery.”
The impetus for changing the system, of course, comes from the insurance companies. “They’re the ones driving it,” says Scherger. “The new HMO or managed-care insurance plans require that a person choose a primary-care doctor. You aren’t free to take the four or five basic problems that you have and say, ‘Well, I want to go to four or five different specialists.’ Insurance companies aren’t willing to pay for that anymore, so they’re mandating this model. And what we’re doing is trying to provide doctors who can follow through with a more efficient, affordable model of health care.”
How big is the swing? “There have been 50 new family practice programs started nationally in the last 18 months, which is more than in the entire decade of the 1980s.” Scherger says 15 percent of medical students are now opting to become “Marcus Welby, MDs,” especially as stories proliferate in med school of specialists graduating, only to find themselves unemployed.
“We focus on the common problems of people,” says Dr. Scherger. “And that means a well-trained family doctor is equipped to handle between 85 and 95 percent of the reasons a person wants to see a doctor. When it comes to keeping people well and treating common health problems, that’s what we specialize in, and that’s what we train for.”
The GP, in other words, is back.
Only this time he’s not the independent shaman with a shingle on his shack. This generation is corporate, with umbilical cords firmly attached to various HMOs. The HMO GP. Standing, by HMO order, between you and the specialist of your choice.
To get his program going, Scherger has set up a family practice clinic right on hospital grounds. That’s where his interns spend half their time.
But the other half, the grueling half, Scherger has them sweating it out in the ER, the psych ward, the geriatric ward, the gyno ward — doing 36-hour stints every three or four days; keeping good, old-fashioned interns’ schedules, the kind that hospitals such as Mercy have long since abandoned as too tough for young docs.
9:00 a.m. Back at the caseload conference. Dr. Marie Shieh, a 29-year-old Chinese-American first-year resident, is outlining her weekend’s most spectacular patient.
“Joan Clayton,” she says. “Her chief complaint is she can’t breathe because of asthma. She’s 21, has had asthma since she was a child. Her mom has cats, dogs, birds, and horses, and she thinks she’s allergic to them. In January she was in a Nevada hospital for infected arthritis of her left ankle. Also had an episode of bronchitis-pneumonia in February. Also has gastric ulcers. She had a suicide attempt in ’93 — took a bunch of theophylline. Surgically, she had 32 teeth removed; she was born with two sets of teeth....”
Heads are shaking.
“I know, it’s amazing isn’t it? She’s also depressed, I don’t know exactly why, but she’s seeing a therapist and she has a psychiatrist. She is currently unemployed. Smoking: When she went to Nevada she started smoking, but she quit. Alcohol: Once in a while. She had three drinks this weekend with her mom. Drugs: She said she just tried pot and crystal but she doesn’t take drugs now. Family: Her dad has asthma and emphysema. The parents did smoke when she was younger, but nobody smokes at home anymore. She said she has had some rectal bleeding. She thinks it’s from her hemorrhoids.”
Dr. Shieh takes a breath. There’s more. “She’s been gaining weight since she was 19 years old, has had a sinus headache for the last couple of weeks, chest pain, and when I got down [to ER] she kept asking for more pain medicine. Vomiting, constipation, diarrhea, burning when urinating, yeast infection. Her skin was warm and moist, she had significant tenderness of her facial area, maxillary and frontal sinuses. Her throat was slightly red, cobblestoned, very little airflow through the lungs. Her sodium was 142, her potassium was 2.9, her white count was 11,400. Her chest x-ray showed scarring in the right middle lobe. She wanted an HIV test....”
She looks up.
“...I’m not really sure what to do with her.”
“I’d send her to Nevada, away from those pets. But then, she smokes there,” jokes Dr. Prabaker. Then he gets serious. “One of the things is education. She cannot go visit her mom, that’s for sure. The pets. Her mom can visit her, but only after a shower or something. It’s those clothes....”
“I told her to wash the cats weekly,” Shieh says. “That might help, but...”
“But just remember,” says Prabaker in his slightly sing-song Indian accent. “When you cannot breathe it’s extremely anxiety-producing. Hold your breath underwater, or just hold your breath! And in a minute what a horrible experience you’re getting, and anxiety causes more shortness of breath, and that causes more anxiety. It is a vicious cycle. You have to break that cycle by giving some Xanax.”
Prabaker hesitates. This man is said to be famous for his uncanny ability to diagnose, especially when symptoms aren’t clear. Nobody interrupts while he gathers his thoughts.
“One other comment. It’s important to realize that mortality is extremely high now among young bronchial asthma patients. It’s steadily increasing. We don’t know why. Some studies say 2 to 5 percent of patients can succumb. You have to be extremely careful.”
Dr. Shieh reads on through other admissions files, most of them clearly indigent — street people — until Dr. Prabaker finally pipes up for my benefit, perhaps embarrassed about the number of homeless people that make up Grossmont’s clientele.
“The patients who come to the hospital...we necessarily do a lot of [tests] on them just to save our skin. And it is an irony. The lawyers are making us do that. In no other country will we do that. We are wondering why the cost is going through the roof? This is one of the reasons.”
“Malpractice,” says Elizondo, shuffling her pile of three-by-five cards of the day’s patients. “The lawyers say, ‘Did you test for everything, absolutely every possibility? Rather than just the likelihood?’ ”
“And most of these patients,” says Prabaker, “come at the last moment, with decay or a very bad heart. They don’t take care of themselves. They come and get admitted, they want everything to be done, so we spend all kinds of money to do everything. Then before they recover completely, they go out, against medical advice, get out of the hospital for their next fix — only to come back two days later.”
Adds Dr. Turnage, “These patients typically have more complicated histories, with medical, psychiatric, and psychosocial problems. What we’re doing is expensive, and it’s very undercompensated.
“My regular patients,” continues Turnage, “don’t have to get a CAT scan every time they get a headache.”
10:00 a.m. Morning rounds. We’re coming down the fire-stairs to the third floor. Jim Turnage and Dr. Prabaker are doing their rounds together. “Marcus Welby, MD. That — truly! — is what I want to be,” says Turnage. He’s got a twinkle in his eye, but you can see he means it. “I’m not interested in being a specialist. People are the most important thing to me. Ever since I was a kid I’ve dreamed of being just this. The doctor in the white coat who looks after regular folks.”
We’re past the nurses’ station, into a room where an elderly woman is propped up on pillows, laboring at her breathing. “Hello, Mrs. Edwards,” Prabaker says. “How are we this morning?” “Congestive heart failure,” Turnage mutters, “asthma, emphysema, pneumonia, fluid in lungs. Exacerbated by diabetes. We use a vibrator to loosen up the sputum. There’s a lot of sputum.”
“You can go home soon,” says Prabaker. “But I very, very strongly recommend you make yourself a patient of Dr. Turnage, here.”
“I telephoned Social Security last week,” says Mrs. Edwards. “Talked to a nice lady, but I only get $452 per month....”
“Well, let’s ask our social services people to work on that, but I think you should continue to follow up with Dr. Turnage.”
“And I’m going blind,” says Mrs. Edwards, as though that might change Prabaker’s mind.
“Well, that’s why you need a regular doctor,” Prabaker tells her. “I’m offering Jim as Mrs. Edwards’s GP,” he says to me, “so he — and our other residents — can develop volume. Jim can take his patients with him when he completes here. I know how hard it can be starting out in private practice. When I began, I had to start from scratch. It was more difficult to gain the confidence and acceptance of patients, partly because I was different in appearance, but today I have a good reputation. And Jim — like 80 percent of doctors training here — he’ll stay in the area. The fact is, the good old family doctor is returning. Isn’t it, Mrs. Edwards?” Prabaker seems to be cheering Mrs. Edwards up. “I was born and raised here,” she says. “Used to work in a telephone answering service. Twenty years. I’ve probably talked to all three of you.”
We’re on our way to Room 311. “I’m not anti-specialist,” says Turnage. “But the U.S. has too many specialists.”
“And our wider perspective is needed,” says Prabaker, nodding constantly to nurses as we walk down the passageway. “Let me give you an example: A young girl, 16 or 17, came into my office with a fever. Rashes on the face. Tenderness on the back. Knee swollen. Her mother said to me, ‘You just do the fever. I’m taking her to a dermatologist for the spots, a chiropractor for the back, an orthopedic for the knee....’ She had not told each of these specialists about the other problems. I said, ‘Let me take care of the patient. I’m not here to take care of the fever, the rash, the knee....’ Because I’m trying to put all these things together. I found her sedimentation rate was 120. Her ANA [antinuclear antibodies] was 128,000. I told the mother I thought her daughter had systemic lupus. Well, now she was fuming at the specialists. But I said, ‘You can’t blame them. Especially if you never told them about the other symptoms.’ But in these cases you need someone general, who has some skills in all the fields. This is why we have the whole trend toward primary care. Because we are far better qualified than a patient to decide if and when a specialist is required, and which one. And of course, that saves the patient money, too.”
Turnage interjects, “All my medical education has been from specialists, but their focus is different than mine. For me, when you divide up a patient into parts, and you just look at an organ system — the skin, or the bones, or the endocrine system, or the glands of the body, or whatever — you lose the patient. And you lose the picture.... You’re likely to miss things. So, for a general internist like Dr. Prabaker, one of his joys in life, and his great expertise, is to look at a whole patient.”
“It’s like the old zebra joke,” says Prabaker. “If it’s striped like a zebra, gallops like a zebra, it probably is a zebra. Common sense plays a big part as well as scientific method. Jim’s patient with the acute inflammation of the gallbladder. Her EKG was abnormal, but she didn’t present with classic gallbladder symptoms. And besides,, she had pulled out her IVs. She wanted to go home. The nurses said she was competent. And according to the law, you have to let patients go. Anyone could have thought it was just pneumonia. Jim had already been on duty 39 hours. He could have said to [Dr. Araya] the first-year intern, ‘You take care of it.’ But something — instinct and training — told them both she was really sick. They telephoned her family to have them convince her to stay. Jim ordered an ultrasound. The radiologist was so impressed he ordered a CAT scan. And there it became apparent. Her gallbladder was gangrenous. It was about to burst! That surgery saved her life. No doubt about it. I’m impressed, really, Jim. Because residents usually don’t have the clinical acumen. This man is one of the best residents I’ve had.”
Turnage tries to swallow his pleasure at the praise. “That’s the thing in this job,” he says. “You really are affecting lives. It’s why I love it. I love being here.”
“It’s also why this trend is good,” says Prabaker. “If you need surgery, we go into the operating room with you, to assist. That way we can evaluate the surgeon. The patient is so grateful that you’re there, and we can see the surgery and the results. If six months down the road there’s further abdominal pain, we are familiar with the situation inside. You see? A nice web. The patient and the doctors are not so isolated as before.”
11:30 a.m. Room 311. Mrs. Lucille Teeter, 84. Also nearly blind. But she’s in for obstruction of the small bowel. A ball of gas in her tummy shows the painful backup.
“I’ve been in ten days and not a bite to. eat and nothing to drink,” she complains. But it’s a joke. In fact, she’s being fed intravenously. Mrs. Teeter has the most beautiful smile. And her eyes, even though they see only shapes now, are blue and clear. What she has is a terrible problem. Five to six bands are stretched across her bowel passage, obstructing the flow of waste materials. “It all started from scar tissue I got in 1929,” she says, “when I had my appendix out.”
“This lady is wonderful. Tough! A true positive thinker,” says Prabaker. “A year ago she had bypass surgery, and she perked up so well that by the fourth day she was out! That shows what can happen with a good positive attitude.”
“Good genes,” says Mrs. Teeter. “And I’m used to trouble. I was born on Christmas Eve, 1909, on a farm in Missouri, in the middle of a blizzard.”
Everybody laughs, but Prabaker and Turnage are worried. Prabaker decides it is time to call in a specialist, a gastroenterologist. As we leave, Lucille Teeter asks Prabaker to stay behind a moment. She wants him to tell her the truth. Is she going to get better?
We haven’t been ten minutes out in the hallway, waiting for Prabaker, when a beeper sounds. A nurse comes out. “Mrs. Teeter,” she says quickly. “She’s coded.”
Suddenly the hallway is awash in nurses running, carrying boxes, doctors and orderlies wheeling gurneys, all toward 311. Relatives appear, looking pale.
“Code Blue,” says someone hurrying by. “ Life-threatening.”
1:30 p.m. “She’s alive,” says Turnage, coming into the hospital cafeteria. He’s got a burger and a salad on his tray. “We’re still not sure if it was a little heart attack or not. We’ve shifted her to the IC [intensive care] floor.”
Turnage has just come from a monthly lunchtime meeting where doctors get together with a facilitator and express personal frustrations with the job. A kind of encounter group for those always coping with other people’s problems.
“There’s a very definite pecking order,” says Turnage, the senior man among the interns.
“The chairman of the department, the senior residents, the junior residents. My job is to guide the junior guys.”
He brings out a little book. It looks like the equivalent to Mao’s little red book. Much thumbed. “This,” he says with mock awe, “is Chan. My bible. Current Clinical Strategies in Family Medicine. It has little mnemonics in it like...SOAP. When [a first-year resident] describes a patient to me, they should always do it in this order. Subjective: What the patient thinks is wrong with him/herself. Objective. What the doctor thinks is wrong. Assessment. His overall feeling as to the patient’s situation. And Plan: What he’s going to do about it. SOAP.”
He flicks to another page. “The other character we come to know well is ADCA VAN DIMSL. I ask what they’ve done about a patient, and they run through ADCA VAN DIMSL: Admit, Diagnosis, Condition, Allergies? Vital signs? Ambulation? Nursing? Diet? IV fluids? Medicines? Special circumstances — like diabetics — and Labs. We do it in that same order till it becomes automatic.”
For an intern, it turns out, Jim Turnage is no spring chicken. He’s 47. In fact, most of his adult life he’s been a Marine or a musician, playing clubs in San Francisco, L.A., and San Diego, even making a few records. He’s originally from Dallas, Texas.
“I’d wanted to be a doctor since I was a little kid. But I couldn’t imagine that I’d ever be good enough to do it. So basically I had to live a fairly long adult life to come to the realization that yes, I could do that.”
He graduated in 1965 from high school, went to Stanford in the “fabulous ’60s,” completed a degree in statistics there, and “in my own personal response to the Vietnam War,” joined the Marines as a flight officer. He was in the back seat of Phantom F-4s. “That catapult launching off carriers — it made me want to be an astronaut, to get that extra kick. It was a thrill in itself.”
When he got out in 1973, after four years in the Marine Corps, he went back to music. He was out there jammin’ all the way through ’86. He’s still a guitar-player and singer-songwriter, still has a little studio in his house.
So how did he make the leap from steel guitar to stethoscope?
“It sounds really mundane, but I analyze my life a couple of times a year — at my birthday in August and the calendar new year; a little brainstorming and prioritizing. One year on my birthday, I did my list, and once again the physician thing kept coming up to the top. So this time I acted. I went to a local college to ask about med school, and they said, ‘You won’t get in because you’re too old.’ I was 36 at that point, 1984.
“But I did it anyway. I went back to school, did all the pre-med courses in 11 months. At that point I was a little out of sync for getting in the application cycle. So I became a high school teacher for a year — in South Central Los Angeles. That was transforming. Locke High School was built right on the site where the Watts riots were in 1965. And it’s everything you’ve ever heard about. We were in Crips territory, lots of gangs, violence — but guess what? I learned something from those kids. If I hadn’t gotten into medical school, I would have stayed there. Every day was a net positive, because the kids somehow would come through, despite all their circumstances.
“Then I got accepted into medical school. A Jesuit school in St. Louis. There was a singular difference in the way it approached medicine. We spent a significant amount of time studying about the bio-psycho-social things that I’m interested in. Typical ’60s.”
Still, he almost went for surgery.
“I did surgery as my first rotation. And I loved it. I thought it was a fascinating, exhilarating experience. I got to assist on an amazing array of surgeries. These are things I will never get to do again in my life. Liver transplants, for instance.
“It seems a bit macabre to people who are not involved in the medical business, but to have your hand in someone’s belly, helping surgically correct something that will allow them to live or palliate their pain, it’s an...experience. Especially if you know the person. Your eyes, your hands, all your senses are involved. The honor to be able to do this. I was so blown away.
“I worry about people who are going through their lives doing things they don’t want to do. I feel really privileged that I’ve been able to do things that I want to do. I truly do this for fun.”
3:00 p.m. Turnage is busy in a cubicle with the Physicians’ Desk Reference. He’s signing someone out, a poor woman who got brain damage in a multi-car pileup. Turnage says she has “profound injuries” to the brain, her awareness of her environment is way down, her swallowing is shot, she tends to breathe down food, she’s subject to pneumonias. Her family has asked for no heroic measures. Her prognosis, Turnage says, is for a “stormy course.”
I wander over to Dr. Fariba Ariz, leaning over the nursing station counter, waiting for a patient’s records. A tall lady named Leslie comes up to her. She’s from the hospital’s social services. “Any luck with Mr. Jones?” Ariz asks her. “He refuses to eat. But there’s not much more we can do. He needs to go.”
“Nobody wants to take him,” says Leslie. She’s talking about board-and-care facilities where she sends patients to convalesce, so they don’t take up expensive hospital space — or end up back on the street, where they often die. “They all say they have no beds, but people like him, they don’t want to take them.” She shakes her head sadly. “It’s a dirty business.”
Mr. Jones, it turns out, is indigent. He has hepatitis C, “end-stage,” as Ariz puts it. A friend from the sheriff s department brought him into Grossmont’s ER.
“Well, keep trying,” says Ariz. She’s 27, looks younger. Yet she’s donning plastic gloves, plastic smock, and a face mask, on her way to see a man dying from an infectious liver disease.
Inside Room 237 you first notice blankets. All you can see of Mr. Jones is a long mass of beautiful brown chestnut hair spread over the pillow. Oprah is blurting out from a wall-mounted television.
“Mr. Jones? Are you cold? We’ll get you another blanket.”
Mr. Jones is sleeping. The exhausted sleep of a body under assault. Ariz leans over, gets Mr. Jones to turn slightly. He’s not an old man, maybe 40. But his face is deep yellow. He’s hardly responding. She touches his stomach. “Does that hurt?” He smiles, perhaps a wince of pain.
“This is not a well-oriented liver,” she mutters.
A few minutes later, outside again, she takes off the mask and gloves. “He’s dying,” she says. “Slowly. He has a very big liver, fluid over the stomach. He’s weak. He can’t eat. And nobody wants to take care of him. He doesn’t have insurance. If he did [the board-and-care facilities] would accept him in a minute. His enzyme levels are worse and worse. Next time he comes it’ll be...”
She doesn’t finish the sentence. This isn’t the first time she’s encountered death.
Back in 1979, 11-year-old Fariba Ariz got used to staring down at dead bodies in the rubble after Iraqi bombing raids. The Iran-Iraq war had come to Teheran.
“Every day we would hear the bombs. When bombing happened they would have airraid sirens that would warn the whole town. But sometimes the planes would come even before the sirens. The first thing you’d hear would be a big shake — the whole ground. Then you’d just run down to the basement, the whole family, and you wait and wait.... Those nights, everything had to be done with candles. Your parents — you got to see them in a different time in their life. You had never seen them facing death before. We became very close. What I saw was not something a lot of people see. You basically see life and death. Any minute you can die.”
That possibility became personal too. Ariz’s father was a top oil executive. With the revolution, there was a worry that anti-Shah rebels would kidnap her because of her father’s position. “I was [put] in a military camp, living with another family, friends of my father, until he thought it was safe. Now when I look back, I’m just happy that I had that experience. Your view to life changes when you see the worst things that can happen. The little things don’t bother you anymore. Your views are a lot different.
“That’s actually what made me interested in becoming a physician. To be able to help my family, and people, wherever they are, in any situation.”
Despite that early experience, she says dealing with patients’ personal crises was hard, especially at first.
“There was a patient in the first month when I was an intern here, an elderly gentleman, and we found out he had leukemia, and he was in such bad condition that he was asking me, ‘Why can’t God take me away?’ That was very hard, to try to tell him to ‘have hope’ and ‘don’t give up,’ seeing him like that and wanting to die. But you learn. I try to use their strength. A patient who is dying, I’ll find out his worst worry, perhaps that his children are going to be without their father, so I try to find the children and bring them in so they can resolve that issue with him.”
Ariz likes the direction American medicine is taking. “In Iran, it’s family practice. Most people have a family physician for life. In the future I think it’s going to be more family physicians too. But it’s tough training to be a doctor here. We have to get loans — $80,000 to $100,000. And that’s without interest. You can imagine by the time you graduate how much interest has accumulated. I just think it’s not fair, realizing that all you do, 24 hours a day, almost, is care for patients, and the amount of money that you earn as a family physician is not enough to be able to pay these loans off right away. Our loan interests are not even tax-deductible. It’s very difficult. I had to take a lot out in loan money. I’ve just been talking to a loan company, trying to defer these loans. In other words, we are very poor doctors.”
Now she’s on her way to the farthest room on the floor. It’s old Mrs. Lassiter. “COPD,” says Ariz, quietly. “Chronic obstructive pulmonary disease. Emphysema. She’s depressed. Her family is not too keen to take her. When I go in she basically cries. She’s worse than discouraged.”
Inside the room, a little lady lies with tubes up her nostrils, breathing shallowly. Ariz puffs her pillows, has her lean forward and breathe as deeply as she can while she listens with her stethoscope on Mrs. Lassiter’s back. “Definitely better,” she says. “You are getting better, but slowly. So we need to be thinking about moving you somewhere where you can get better. A Transition Care Unit.”
“Oh no!” says Mrs. Lassiter, panicking. “I went to one once. They were rough and rude and crude. The nurses had no compassion. I don’t want to go to one of those places! I want to stay here.”
“If you stay here, we’ll have to send you home,” says Ariz. “We can’t do any more for you. You’re getting better. Truly.”
Tears are rolling down Mrs. Lassiter’s cheeks. Her strained breathing is fitful. “I don’t want to go today, because...I’m not ready! I don’t want to be pushed around again. Can’t I stay till tomorrow?”
“I think we have a deal here,” says Ariz. “You agree to the TCU — it’s just downstairs — and we’ll let you stay here tonight.”
Mrs. Lassiter takes a long breath. “Would you talk to my daughter?” she asks Ariz.
As the day wears on — and it is a long one, constantly on your feet, constantly talking with people in trouble — it becomes apparent that all the interns here are unusual people. Unusual in their outlook, unusual in the journey that brought them to this profession.
Alberto Araya, of crunchy gallbladder fame, is passing through on his way downstairs for 12 more hours in the ER. Araya, in his 40s, also came late to doctoring. He’s from Chile and has had a family to look after for 20 years. Like Jim Turnage, it took until his late 30s before he could find the time to study medicine.
Marie Shieh, on her way back from the psychiatric ward, says she became a doctor “to spite” her family, because they wanted her elder brother to take on the task. “But my father did always want me to have a career so I wouldn’t be dependent on a husband,” she says. “They were pleased when I graduated. They never expected it out of [their daughter]. Asian people push their children. They want their kids to be respected.”
Marie is married to an (Anglo-American) acupuncturist, whom she met while she was teaching for a year in provincial China. She wants to set up a dual clinic with her husband, offering medicine from “both worlds.” She “has a big social leaning” and believes in socialized medicine, such as the Canadian single-payer system. She thinks doctors are overpaid and would like to go work for the World Health Organization one day. Yes, the interning is hard work, she says, but “I just love to come in here to work. It’s like a drug. Only thing is, your spouse has to be extremely understanding.”
But the job carries its share of horrors and doubts. Shieh still tortures herself over a patient who “died on me” — an 83-year-old lady who came in with heart problems. “It was 5:00 in the morning. I was tired. She looked in good shape. We talked. She was alert, intelligent. I liked her. We did an electrocardiogram, and I suddenly realized her heart was a ticking time bomb. Half an hour later...she was dead. Aneurysm in the aorta. It had burst. I go over and over that morning, thinking, ‘If I’d been quicker....’ ”
5:00 p.m. As I walk out of the hospital and down to Grossmont Center, leaving all these personal dramas behind, I think of myself at Ariz and Shieh’s ages, late 20s, committed to — what? A good time? A general plundering of the world’s riches? Is it because this group of interns are minority Americans that they have stronger values of family and duty than I ever had?
It looks like this crowd of new doctors will give it back, in spades. And if they’re heralding an era when doctors are encouraged to be “people” people, as opposed to scientists looking for lab rats, that has to be a good backward-step-forward for American medicine.
But as I prepare to enter the world again, I remember Dr. Turnage’s last words:
“If you’re going to get sick, for God’s sake don’t do it July 1.”
I asked him why not.
“Because that’s the day the new year’s intake of interns starts,” he says. “Believe me, they’ll all be very nervous.”
Comments