{kind=link}
Here's something you might be interested in.
Ask a Hipster — Advice you didn't know you needed
Big Screen — Movie commentary
Blurt — Music's inside track
Booze News — San Diego spirits
Classical Music — Immortal beauty
Classifieds — Free and easy
Close to Home — What it’s like on the street where you live
Cover Stories — Front-page features
Drinks All Around — Bartenders' drink recipes
Excerpts — Literary and spiritual excerpts
Feast! — Food & drink reviews
Feature Stories — Local news & stories
Fishing Report — What’s getting hooked from ship and shore
From the Archives — Spotlight on the past
Golden Dreams — Talk of the town
The Gonzo Report — Making the musical scene, or at least reporting from it
Letters — Our inbox
Movies@Home — Local movie buffs share favorites
Movie Reviews — Our critics' picks and pans
Musician Interviews — Up close with local artists
Neighborhood News from Stringers — Hyperlocal news
News Ticker — News & politics
Obermeyer — San Diego politics illustrated
Outdoors — Weekly changes in flora and fauna
Overheard in San Diego — Eavesdropping illustrated
Poetry — The old and the new
Reader Travel — Travel section built by travelers
Reading — The hunt for intellectuals
Roam-O-Rama — SoCal's best hiking/biking trails
San Diego Beer — Inside San Diego suds
SD on the QT — Almost factual news
Sheep and Goats — Places of worship
Special Issues — The best of
Street Style — San Diego streets have style
Surf Diego — Real stories from those braving the waves
Theater — On stage in San Diego this week
Tin Fork — Silver spoon alternative
Under the Radar — Matt Potter's undercover work
Unforgettable — Long-ago San Diego
Unreal Estate — San Diego's priciest pads
Your Week — Daily event picks
Tijuana coroner's patients cut and sawed open
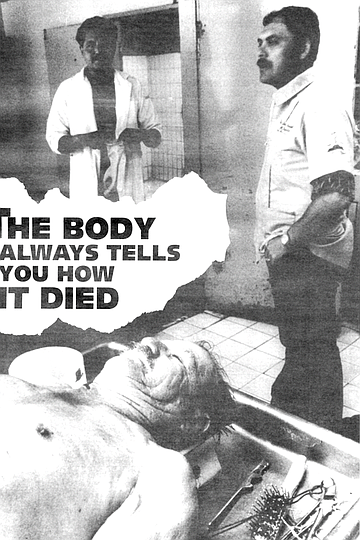
The body always tells you how it died
Many of the names on the chart read simply Desconocido, Unknown, Juan or Juana Doe.
The house of death in Tijuana is the color of dusty bubble gum. Just off the Plaza Club de Leones, with its cathedral-like tower, where Revolucion curves away to the north, SEMEFO, the one-story coroner's office, sits atop a low hill at the end of a sand and cobblestone drive.
I notice that her brain appears fake. I have seen more realistic-looking brains in horror movies.
SEMEFO stands for Servicio Medico Forense, Medical Forensic Service. The dust rises from constant street repairs, from wind that rakes the sand across the cobblestones, and comings and goings of white vans marked D.I.F., with SEMEFO spelled backward beneath the windshield. The vans arrive with a cargo of dead passengers and leave empty.
Technicians greet the drivers at a gate of hurricane fencing and plywood painted gray. The vans back in, the gate is closed, but not before revealing a glimpse of dirty yellow oilcloth or Leatherette curtains that will be pulled aside to admit clientes, as the technicians call them.

The tech presents the left lung in his cupped, gloved palms. Corona points out a black filigree on the organ and pronounces, “Smoker.”
The waiting room is a faded pink, with some of the same charcoal paint used on the gate. Three potted plants seem in need of water. An unframed painting in gaudy golds and muted browns of a galleon at sunset has been punctured at its center.
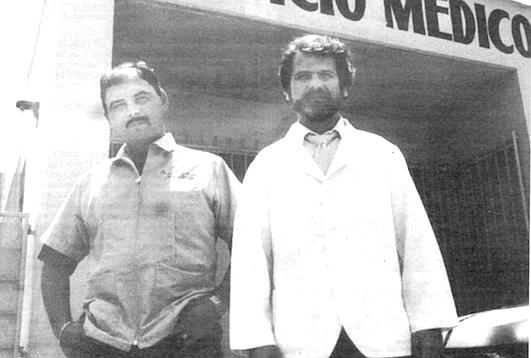
Doctors Amador and Escajadillo. "There is no such thing as the perfect crime."
The kind of sluggish flies that seem to hover in the dead center of a room in Southern California and Baja in the spring trace lazy spirals and arcs, scattering when someone in the waiting room rises to make an inquiry at the glass partition to the inner office.
Behind me bodies are being removed from the walk-in refrigerator where they are stacked on trays.
The walls at shin level are scuffed and imprinted with small, dirty palm and finger prints. A poster framed under cracked glass has a rose in a clean ashtray with the words Gracias Por No Fumar.
“You will see every type of behavior in this waiting room.”
Manning the desk behind the glass partition is a boy, possibly 20, with a complexion problem, wearing a khaki uniform, a flat-topped haircut, and shiny black-laced shoes beneath frayed pants cuffs. His brass nameplate reads M. Radillo. He answers the phones, makes notes on a clipboard, and enters names in grease pencil on a white plastic wall chart: today’s lineup of clientes.
I see a burn victim that is unrecognizable as either man or woman.
Many of the names on the chart read simply Desconocido, Unknown, Juan or Juana Doe. The chart indicates the time the bodies arrived and were logged in, the date, the day, and their origin, whether it is the street, the prison, or a hospital. “Customers” come routinely from Rosarito and from as far away as Ensenada.
In the waiting room are three women, representing three generations, clearly, of one family. Two children play on the floor, one with a key ring, the other with an empty plastic juice bottle. None of the women are crying or seem visibly upset, though they ration their smiles to the children and the two men who stick their heads into the room every few minutes, between cigarettes. The women do not smile at each other.
“You have a relative here?” Iask.
“Yes,” the young mother nods and says nothing more. Possibly they weren’t close to the relative, but I suspect their lack of apparent grief has more to do with a cultural imperative. Just a few miles north, death always takes place offstage. It is almost always a tragedy and a big goddamned surprise, a dirty trick, unthinkable.
Brain hemorrhage,” says Doctor Corona, a diminutive man in his late 50s or early 60s who wears eyeglasses, a white lab coat, and hair dyed to match his toupee. “This lady has high blood pressure.” He points into the opened skull to a mottling of clotted blood in the top of the left brain hemisphere. “A vascular accident!” he declares with finality.
The woman is a Jane Doe, approximately 45 years of age, with two front teeth of silverish metal that gave her plump carcass the look of a large, flayed rodent.
The handwriting in my notebook is not as shaky as it was several moments ago. When I walked into the room and saw the two corpses (a third one “on deck” on a tray to the left), my reaction was immediate, clear, and probably shameful. I thought. I'm glad it’s them and not me.
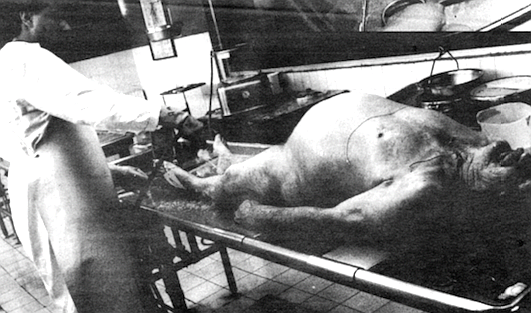
The room is rectangular, longer than it is wide, with two chromium tables fitted with slightly sunken drains at their centers. The bodies lie on chrome slats elevated from the pan of the table. Heads are rested on plastic hourglass-shaped blocks. The body on the second table is that of a fat man. His hair is thin, dyed black. He has a mustache. A technician holds a long metal cylinder attached to an amber surgical tube that is in turn connected to a machine: a glass container with several inches of urine-colored fluid at its bottom. The tech has the cylinder or rod inserted into the dead man’s side, just below his rib cage. There is a livid incision just long enough to accommodate the rod. The tech is jiggling the device, working it into the cadaver, causing the dead man to writhe in an undignified way, his thin strands of hair swaying out of place. It is as if the corpse is being tickled, responding with galvanic convulsions of silent mirth he is helpless to stop.
It occurs to me that for some reason the tech is draining the body’s bladder of urine, though I can’t think why this would be done. I am fighting an urge to giggle because it would be inappropriate — all laughter ceases when the doctors, the coroners, enter the autopsy room — and because I am certain that the giggle would escape at a higher pitch than I would like to hear coming from my own throat.
“What is that man doing?” I ask Corona.
“He is preparing the body. There will be no autopsy. Cardiac arrest.” Corona seems uninterested in the case.
The man is being embalmed. I now notice that the level of yellowish fluid in the container is dropping, not rising. He is being pumped full of a formaldehyde-based solution.
This procedure had distracted me while the Jane Doe had been opened from trachea to pubis with a scalpel, revealing an inch or so of fat the color of custard along with her sternum and rib cage. The breast bone was cut by the technician wearing ivory rubber gloves of the type you might wear if you were particularly fastidious while cleaning your bathroom. To cut the chest, the tech uses not a medical instrument, but a garden tool, something with which you would prune a rose bush. The ribs were snapped quickly one after another, the sternum came away in a triangular shape still hinged near the clavicle. The technician bent back the sternum suddenly toward the woman’s face, and it came away in his hand with a snapping noise like someone cracking his knuckles loudly.
I am breathing through my mouth from necessity.
The tech presents the left lung in his cupped, gloved palms. Corona points out a black filigree on the organ and pronounces, “Smoker.” He points with a pen. He does not touch the body; only the technician touches the body. In the next moment the tech is almost up to his elbows in intestines, but not before he has exposed the heart with an abnormally thick layer of bright yellow fat around it: the stuff you trim away from a whole chicken before you roast it.
Corona’s pen points like a divining rod toward what interests him. He takes care not to make contact with the organs, the body, the wetworks, Jane Doe. I am again fighting a slight case of hysteria. I think to myself about Corona, At no time do this dark magician’s hands leave his arms, folks. To cover my discomposure I jot down a note. Thinking of the woman’s approximate age, only three years older than me, I write, “Death seems to age you...or poverty. Maybe poverty and death...” and I lose it. I start to giggle like a schoolgirl catching her first glimpse of a boy’s weenie in the nurses’ office — and it wasn’t what she expected. I cover this immediately by making coughing noises.
“Are you all right?”
“Yes, yes. Sorry.”
After digging through her lower intestines, examining the liver (good, not a drinker or drug user) and kidneys (normal), the tech exposes (scoops out, really) her bladder and uterus; long, straight pubic hairs over a hollow shell where incredibly compact and ingeniously devised reproductive and eliminative soft machinery has been removed. Corona announces, “Now we will look at her brain.”
The tech wrestles the woman’s head back onto the hourglass and places a scalpel beneath her right ear. He makes an incision around the back of the skull and completes it just beneath her left ear. He peels the scalp away like a grape, a banana, a pliant coconut rind. He pulls the front half of it over her face like a stocking cap and reaches for the hacksaw.
Blood, a viscous burgundy, drips slowly onto the gurney.
The tech, whose name is Gustavo, begins to saw in a straight line from her crown toward her ears. My stomach lurches in rhythm with the damp wheezing sound of the blade. Bits of pulverized bone, like sawdust or light snow, fall into the dark pool of blood and onto the surrounding chromium.
I see my reflection in a panel of glass that runs the length of the autopsy room. Beyond the glass I can see the “amphitheater,” several long benches, rising like bleachers, where medical students observe autopsies and hear lectures.
Now Gustavo is sawing in a line that reaches across the woman’s brow. In about a minute, the saw meets the first cut at the top of the ears. Gustavo lifts away the exposed skull, which comes away reluctantly with a sucking sound. He takes a scalpel and cuts at the grey cerebral membrane that clings to the inner skull and brain hemispheres.
Behind me bodies are being removed from the walk-in refrigerator where they are stacked on trays. Many are the bodies of old men, thin, with wispy grey hairs everywhere on their bodies. They all have in common: flattened buttocks and “lividity” or reddish purple mottling of the skin along their backs and buttocks, the undersides of their arms and legs. This is a matter of gravity, the blood settling at the lowest point in the body when it is no longer being circulated.
Turning back to Jane Doe, I notice that her brain appears fake. I have seen more realistic-looking brains in horror movies. This reassures me. Corona points to the left hemisphere and makes his pronouncement about the vascular accident. “She probably eats too much grease.” He nods, satisfied.
Gustavo lifts out the brain. It is slightly larger than his cupped hands, the size of a cantaloupe and flattened at the base. He places the brain into the metal scale suspended over the table and weighs it. It looks to be a little more than a kilogram. A few more measurements are taken, organs weighed. Corona makes notes on the form he has in his clipboard, and the autopsy is completed.
Outside, I draw in lungfuls of air and dust through my mouth and nose. It is delicious, like pepper and salt, orange juice, wine...anything.
That night I dream that Jane Doe is dancing with the embalmed man with the dyed hair. Her right arm is over his left shoulder and poised in rigor as though palsied or in an invisible cast. Her scalp is still peeled over her face, the forward hairs or bangs now a walrus mustache above her two metal rodent teeth. The man shakes with laughter, jiggling like Cab Calloway singing “Reefer Man,” as the couple performs the Forensic Four Step, the Post-Mortem Pavane. In the background Fred Astaire sings, “Heaven, I’m in Heaven...and I hardly feel the ground beneath my feet...” Juana says, “I’d like my face back now. Can I have my face back now?”
Dr. Jesus Ramon Escajadillo, 39, is a handsome man with blue-green eyes and a beard with nascent traces of grey. Today he is wearing a black cowboy hat, striped necktie, and white lab coat. He examines the lineup on the wall board and asks me if I have gotten permission from medical director Dr. Gustavo Salazar to observe an autopsy. I tell him yes and that I’ve already observed one.
“We just don’t want a story about bad doctors in bad conditions doing bad work. That would cause us problems. It would cause me problems, and then that would cause you problems. I know this place doesn’t look good. You could write about the bathroom here alone, never get past that and people would say, ‘Yes, a Third World coroner’s office, it’s terrible.’ We.don’t have the same facilities here as you do in San Diego. But we take our work very seriously. In four months — it has been approved — we will have newer, better facilities here. Construction will begin soon.”
Escajadillo takes his clipboard into the autopsy room and beckons for me to follow. Today, a Monday, the room is filled with corpses. I fight down panic and a rising machaca burrito breakfast as I see a burn victim that is unrecognizable as either man or woman. It is human only in the sense of a charcoal parody done by some grotesque sculptor. Beneath the barbecued head, arm and leg stumps, and torso are lumps of briquets, carbonized calves and feet that are arranged on the cart to suggest where they originally belonged. They could as well be burnt pieces of the building the victim was unearthed from, as far as I can tell.
Next to the burn victim, on the same cart, is the body of a child, maybe three years old. The cadaver is plainly that of a boy with golden hair. One eye is swollen shut and bruised, the color of jacaranda blossoms. “Orbital hematoma,” Escajadillo calls it. Bruises on his legs and arms are apparent, and my first thought is that this kid was beaten to death, but I am wrong.
“No,” Escajadillo says, “he fell, I believe. Five stories from a window.” The child looks angelic. I think of Eric Clapton’s son, then of Studs Lonigan, “Live fast, die young, and leave a good-looking corpse.” Girlish laughter threatens to erupt from my throat again, but it is stifled as if a gimlet were driven into my esophagus by the sight of an infant, possibly six weeks old, his nostrils caked with a white crystalline foam. “What...?" I begin, but Escajadillo shunts me over to the first autopsy at hand. “I don’t know about the infant. We’ll see. First we have this man.”
The customer at table one is “Approximately 25 years of age,” Escajadillo intones into my tape recorder. The body is that of a healthy-looking man in his prime with no apparent evidence of trauma. Black hair and mustache. He is muscular. “According to the information we have from the ministry, he was in a traffic accident. He was riding a motorcycle. He came in at,” he checks his clipboard, “16:30, 4:30 yesterday afternoon. This one,” moving to table two, “is a possible drug overdose. We will run studies to make sure. You see, he is approximately 35 years old.” The man at table two has much grey in his hair, is clean shaven, handsome except that he is as dead as two-toned spats and has foam sluggishly erupting through his nostrils. “Bronchial aspiration,” Escajadillo describes it. “We must find out why.”
A little blood mixes with the foam that had been forced through his nose from his lungs. “He was found on the street," Escajadillo says. The doctor’s guess about overdose seems like a good one. On the cadaver’s right arm is a tattoo of a marijuana leaf. Another tattoo reads P.O.P.E. On the left forehead is dust from the street where he had lain.
With a seamstress’s tape measure, Gustavo, the tech, measures the body’s shoulders, thorax, and abdomen and calls out the measurements in centimeters. Escajadillo writes down the numbers on his form. The body is five meters in height. “The foam tells us, in an indirect way, that the patient died from bronchial aspiration or lung aspiration. But why?"
The tech makes the long incision from the throat to pubic hairs. The lips of the incision peel away from each other with relieved tension, as though his skin had been stretched too tightly over his body. Again a layer of fat, but much less of it than on the Jane Doe. Escajadillo peers into the trachea, pointing with his pen. Gustavo leans over and with his scalpel opens the trachea farther. More foam and more blood. His scalpel flicks a droplet of blood onto the coroner’s white lab coat. The doctor backs away saying, “Hey! Hey!” and then laughs. Gustavo laughs and apologizes.
“From the tattoos, the maguey plant? No, a marijuana plant with the name Toni above it, and this one,” points to the second tattoo on the lower right arm, “we might assume he is a drug user whose name is Toni or Pope” (po-pay). “We will look in his liver, his stomach, heart, and kidneys, and we will run some tests.” Escajadillo makes a notation that the “patient” has two tattoos on his left side. They are in fact on his right side, but I do not correct him.
“I can’t see any sign of trauma or violence. There is an abrasion on the knee that occurred eight to ten days ago.” Looking into the mouth. “Teeth are incomplete.” He writes this down. “Male, regular complexion, eyes brown, forehead wide, his mouth is regular, teeth incomplete, no mustache. Between 35 and 38 years old. Chin is square, regular ears. Now sometimes you cannot see any signs of trauma on the outside, but will discover a hematoma inside. This is clean, no trauma. Internal hematoma looks violet in color with a little bit of blood around. Let’s have a look the heart.”
Gustavo is cutting away at the protective tissue around the heart. A pale, bloody fluid escapes. “This liquid is normal. We can have as much as 16 milliliters of liquid around the pericardium, so he is normal here. Not too much fat around the heart, but you can see here,” he points with his pen, “you can see here in this small coronary artery, signs of arteriosclerosis.” He is pointing to what looks like a pinprick along the surface of the heart. I would never have seen it. “It means his levels of cholesterol were probably high, but there are no signs of a heart attack at least in the anterior compartments. Now we'll have a look at the posterior compartments...” Gustavo flips the heart in his hands, exposing the B side. “Posterior compartment is clean. No signs of recent heart attack. Now we have to look at the lungs.
“Now this man is a smoker, this is called anthracosis.” Later, looking up the word, I see that it is derived from anthracite and literally means the condition derived from inhaling coal dust. “You see this, these spots of blood? We call these Tardieu spots in forensics. These spots tell us that this man had severe hypoxia [lack of oxygen] before death, which is compatible with what we see there with the foam. We are pressing the lungs, you see?” Indeed Gustavo is squeezing the purple-and-black mottled organs like bellows. More bloody foam erupts from the patient’s nostrils.
On the next table, the cadaver of the 25-year-old has been opened, his skull peeled away. The smell is much worse from this corpse because of the amount of time transpired between death and refrigeration. The doctor in charge of that case is Dr. Amador. I ask Escajadillo if the smell ever gets to him.
“If the body has been dead for weeks, it can get bad. This isn’t bad. This man,” indicating the bronchially aspirated man, “has been dead less than 48 hours.”
“So you get used to it?”
“Yes,” he shrugs. I don’t believe him. I can’t imagine getting used to it, but no one else in the room seems uncomfortable. “Look here,” pointing to the opened throat on the body, Toni or Pope. “The trachea is full of secretions. You see the foam coming out? Now let’s check the liver. It seems fine. This is the spleen. Fine. Now here is the stomach... you can see here several things,” but he is not pointing to the stomach but to the small lower intestines that Gustavo presents by the handful like long, thin balloons or pale sausages. Escajadillo assesses the organs with what appear to be almost cursory glances, but he knows what he is looking for. “This man has intestinal bleeding from the small bowel. You can see the discoloration (a dark section of tubing] in this section of the lumen. There is a gastrointestinal problem with this man.”
Examining the pancreas, the doctor seems satisfied. Behind me. Dr. Amador’s tech has started sawing the skull of the motorcycle accident victim. The sound sends my stomach into fitful lurches again. To shift my focus, I ask Escajadillo if he could venture a guess at this point as to the probable cause of death of his “patient.” He smiles and shakes his head, “We don’t guess,” he says.
Gustavo exposes the kidneys. The left one seems normal, but the right one is at least twice the size of the left. “We call this hydronephrosis.” The examiner instructs Gustavo to open the stomach. Gustavo takes his scalpel and punctures the bladder, tears it, the way you might open a bag of potato chips with a letter opener. I peer inside at a green fluid. “Bile?” I ask wrinkling my nose.
“Salsa verde.” Escajadillo smiles. “It went up to his throat, to his trachea, causing bronchial aspiration. There is bleeding and edema in the small bowel. Several things may have happened. He may have had intestinal infection which caused him to vomit, which in turn caused the aspiration. But a lot of us have infection, throw up, and cough, but we do not die. So why did he die? Besides the intestinal problem, he has the hydronephrosis of the kidney. Two pathologies we can see now this patient had. We have to be sure he did not also ingest alcohol. We will run tests, primarily blood tests, but we will run a sample from the stomach for drugs or infection. Mostly we must quantify the blood alcohol level and test for certain drugs. After this lab report, we will be able to determine what is acceptable as the cause of death. But we have an idea now.”
“Food poisoning?” I ask.
He nods, “That is possible, that is why we are going to run the contents of the stomach. Make a culture. It takes about three or four days. I am going to make my preliminary report that the cause of death was bronchial aspiration. I will sustain that pending the results from the lab tests. You see? We have to wait.”
A forensic chemist comes every day to take away samples to be tested. He is paid by the state, a member of the forensic department, referred to as the ministry, the umbrella office of the state police.
Again with the saw, Toni’s brain is opened. “We have to look for trauma or congestion,” Escajadillo says. “We have to be sure that the brain has not been involved in violence...trauma. There is some cephalic congestion, you see,” In fact, I do not see what the coroner is seeing. Possibly it is a purplish clotting of blood to the left of the left hemisphere. “Probably because of the hypoxia.” We wait while Gustavo removes the section of skull. I ask why no one is making jokes the way you see medical examiners doing in American movies. “Well, sometimes, “ the doctor says, “but we do not joke at the expense of the body. Sometimes we will joke about the situation in the examining room or events that surrounded the death, but in general we try to be respectful.
“You see our electrical saw is not working,” he points to a white circular saw sitting off to one side.
“The blade is not sharp enough. We’re waiting for new blades. The hacksaw is good, but we have to improvise often, like the shears. Whatever works is fine. We’re not dealing with living tissue.
“We would like to have a little more good equipment, of course. That would help. We even need a new pair of scissors. If we could change the equipment every year, that would be great for us, but sometimes it’s just not possible. We’re working on it. You see the congestion here. We need more space.”
The word “congestion” seems to remind Escajadillo of the job at hand. He points to the brain again with his Bic Fine Point. “This is compatible with all the signs we saw in this body. We can see some periosteal seams, another sign of hypoxia. Now we will take out the brain, see if there is any sign of skull fracture or hemorrhage in the ventricular system of the brain. We want to remove the dura, the membrane, so we can see the bone and any irregular lines, like cracks. Here we can see the anterior compartment, the olfactory nerve, the roof of the ear, the fifth cranial nerve, the third cranial, the hypoglossal nerve, the optic chiasma...." As the litany is intoned, Gustavo draws blood from the empty brain pan with a hypodermic the size of a turkey baster. “Here is the seventh cranial nerve which moves the face. The eighth governs hearing and vestibular function...not to be dizzy, you see?”
Again Gustavo accidentally spatters a little blood on the coroner. Escajadillo laughs and in mock outrage says, “Hey hey hey hey hey!”
He introduces me to Dr. Julio Javier Amador Barragan, who is conducting the autopsy on the hapless motorcyclist. Amador is 32, with a round, pleasant face. He wears a blue smock instead of a white lab coat.
“A motorcycle accident,” Amador begins. “He has trauma to the brain and the thorax. Brain hemorrhage and lung hemorrhage. We will examine the abdominal wall and cavity.”
Since Amador has established two separate causes of death, why look further?
“Although he has damage to other organs, we know that the damage to the brain is not compatible with life. He might have survived the trauma to the thorax. He was a smoker, and this discoloration of the lungs indicates that his lungs were attached to the ribs. This individual had chronic lung disease. We cannot establish at this point if he was exposed to tuberculosis or some other form of disease.”
He wasn’t wearing a helmet?
“It is not established in the reports we have, but I can assure you it is uncommon for these guys to wear helmets. He was not wearing a helmet. We don’t know his name. The reason we keep looking beyond the possible or probable causes of death is that there may yet be others. Even something you would think as obvious like a gunshot wound can be so small you cannot sec it clearly. There have been many cases where an individual has been killed and then has an apparent car accident. You have to look for further causes. We are obligated to the police department, the justice system. This is one reason, simple thoroughness is another."
I venture my theory that the Juan Doe had a coughing fit while riding his motorcycle and crashed into something.
“We cannot determine that. We would need a crystal ball to establish he was coughing before he died. We can establish, because of the fibrosis and the lung’s attachment to the ribs, that he had a problem. Whether the problem had anything to do with the accident, we can’t say.”
“Sounds like his number was just up,” I say, but Amador looks puzzled, as if he doesn’t know what that means. Certainly I don’t either, so I say nothing more.
At this point Escajadillo calls my attention back to the previous autopsy. “We are weighing the kidneys,” he announces as if this is something he wants noted. “The one on the right side weighs 200 grams. The one on the left is 150 grams. We have trimmed all the fat tissue away. You see the difference?”
Escajadillo moves to the charred corpse and signals me. “This is Doctor Quiroz.” He indicates a pretty and full-figured woman in a lab coat. “This is her case. Looks like 100 percent burns, say 98, we still have some tissue at the right breast. Usually this happens at home. Maybe she was living in not very good conditions and was trying to get warmer at night. Maybe she tried to burn something for heat, and the whole house, whoosh! This is more common in the winter, but there could be other causes. Some criminals when they want to get rid of someone and they shoot or stab someone, they will burn the body. They think by doing this we won’t find out what really happened. In each burn victim — we study them, take X rays, everything.”
In a body this badly burned could the pathologists find gunshot wounds or stab wounds?
“Yes. We will find it. The general rule is...”
Here Amador interjects happily, “The body always tells you how it died,” and smiles at Escajadillo.
“Yes. The body is always trying to get your attention. You just have to be sensitive to the correct diagnosis.”
What percentage of bodies that come in are victims of violence?
“We have statistics from last year [1992]. The main reason of death is trauma, mostly related to accidents, number two is heart attack, the third leading cause of death is due to firearms, the fourth is bronchial aspiration, the fifth is death related to the use of knives. We call those arma blanca or white-arm killings. The rest is gastrointestinal, like cirrhosis, liver problems. Now with the summer we will have a lot of drunk people, alcohol-related deaths.”
What happens when Americans come down here and die? “By law we have to do the autopsy here. We can’t send the body to the United States for an autopsy because the Mexican authorities have to be informed by the same system here in Mexico as to what was the cause of death. The explanation for this is simple if you think about it.”
Amador then points out to me that his motorcycle rider has traumatized kidneys, though I cannot detect the damaged tissue or distinguish it from healthy tissue. He will also order blood tests and stomach cultures.
Escajadillo moves to the child who had fallen out of the window. “See, he fell from a fifth floor, but he survived a little bit afterward because we see medical sutures.” He points to stitches on the child’s neck. “And we see here an injection mark, a puncture at his ankle where he was given saline or blood or something, some IV fluids. I think he was two or two and a half.”
'The infant on table four, possibly a month or two old, is several feet away, the province of Dr. Quiroz. Escajadillo looks at the tiny boy and points out the crystalized foam around its nostrils. “Bronchial aspiration again.” He points to yellow-green stains around the child’s bowels and genitals and says, “This liquid staining makes me think a respiratory or gastrointestinal dysfunction. We will not do an autopsy, the public minister does not require it. There is no question of any crime related to the death." Escajadillo’s dismissal of an autopsy seems to be borne out of a reluctance to desecrate the body of an infant, possibly weighing what forensic science would learn against the abhorrence of mutilating something otherwise perfect. I am speculating, but I sensed Dr. E. did not want to dwell on this case.
“Is there any indication,” I ask, “that the death might have been prevented?”
“It is very hard to say. Sometimes when the parents are concerned about a common cold, the child may die anyway. Sometimes the parents are negligent, a lack of concern, but this is impossible to say in a case like this. So what is the point?”
The coroners dismiss me as the autopsies are completed. I wait in the driveway sucking lungfuls of air as two well-dressed men in their 30s emerge from the medical director’s office. They are reporters from El Mexicano, the Tijuana daily newspaper. They are, they tell me, following up a story on the likely murder of two prisoners by federale officers in the T.J. pen, the Casa Blanca.
“One of the guys has a fractured skull, the other one, we don’t know or they won’t tell us. They said come back tomorrow or the next day.” This was something I had been told for days while waiting to get inside SEMEFO. “It is a very dark business. Maybe you can find out something.”
Indeed, I ask Amador and Escajadillo when they emerge from the autopsy room around 11:30 a.m. They must both resume their private practice for the rest of the day; Escajadillo as an ear, nose, and throat physician and Amador as a general practitioner.
“Yes, one of the prisoners had a fractured skull,” says Dr. E. “The other one, I don’t know. It’s not our case, and I don’t know if we’re supposed to say anything.” He looks at Amador, who shakes his head.
“No, says Amador, we can’t say. You will have to talk with Dr. Salazar.”
I ask Amador about the unhappy people in the lobby.
Relatives of the deceased? “Very often. Sometimes people are just looking for someone who is missing. This is the last place you look because it is the last place you want to look, of course. Some are here to be certified for wounds or injuries that occur in violent situations. We don’t treat them, but we look at them and certify that they have such-and-such lacerations, contusions, or abrasions, how long it will likely take to heal, and things like that. We sign the papers and they go back to the D.A., who gives the certification to the judge. We work with people who are alive too.”
Escajadillo adds, “You will see every type of behavior in this waiting room.”
Jesus Ram6n Escajadillo has been in forensics for seven years and claims, “I would do it even if I were not being paid. It is like my hobby in many ways. It makes me a better doctor, and I am always fascinated. No one does this just for the money. I can speak for 100 percent of the doctors, I believe. Forensic pathologists in the United States make many times what we are paid to do this one week out of every month. Well, we end up working more than that with court time and everything.”
Escajadillo considers himself a medical scholar, his ENT practice enables him to “survive,” and he adds “something more than $12,000 a year” to his income by his work at SEMEFO. He studied in Mexico City and then served a fellowship in Holland for two years studying thoracic surgery. He trained for another two years in Tijuana as a forensic doctor.
Why would anyone seek out this work? How can you get used to this, much less love it?
“You have to have a special interest, a predisposition. I can’t explain it. Look, I have been here for several years and sometimes...mainly, mainly with the kids...I can’t understand...it’s very hard for me to see...people who didn’t have any reason to die. People crossing the street and a drunk kills them, that’s hard. But children especially...children. It’s hard when you deal with a body who has been decomposing for a long time. Not easy. I’ll tell you. But I feel like I’m helping the community. I’m part of the community, and we are, all of us, moving into the next century and I feel a part of it.”
Amador’s interest is in “enforcing the law. This gives me an opportunity to learn how much violence there is in my city and that something is being done about it or maybe nothing is being done about it. If nothing is being done in a particular case, it is not because of me. We see cases that were misdiagnosed, and it is our job to say so, even if this does not make us popular with the medical community here. Sometimes we are considered, by other doctors here...ahh...”
“Pains in the ass?” I suggest.
Amador smiles. Escajadillo illustrates the necessity for the Tijuana Forensic Office’s services with a case in point. “There was a female patient — excuse me for saying patient, it is a habit — she was the mother-in-law of a guy who lived here in Tijuana, though she lived in, I think, Chula Vista or National City. The mother-in-law didn’t like the son-in-law. She had a very prosperous business. Her son-in-law was working with her and he got fed.up with her behavior. He tried to make the perfect crime of her.
“Some of the neighbors of the woman heard an argument with her and the son-in-law that ended abruptly. He stabbed her about 250 times. He tried to clean up all the blood and take the body to Tijuana. He put her in the trunk and went to la presa, the reservoir. He put gasoline and kerosene in the car, and everything was completely burned. The police sent us small burnt pieces of this lady. You saw that burned lady this morning? That was nothing. Anyway, we found something was very much wrong with this burn victim; wounds that were not compatible with a car accident and fire. We found lesions and trauma to the bone fragments. We told the police here, ‘This was a crime.’ So they contacted the SDPD liaison guy and found out that they were missing a body in what was obviously a homicide of a brutal nature. We gave them the autopsy report, and they put this guy together with the victim.” Did they arrest the guy?
Dr. E. looks at Dr. A. quizzically. “Yeah, I think they got him. We handed them everything.”
Dr. A. says. “I think they made the arrest.”
“You see?” Escajadillo says. “We need better communication with the other side. We should have meetings once a month with the forensic guys in San Diego and theTJ guys. We share the same problems, the same crimes, the same criminals. Half the time our victims are related to somebody with a file on the other side.”
Amador leans forward, “You see, his story tells you. There is no such thing as the perfect crime. The body always tells you how it died.”
“No such thing as the perfect crime?” I ask both of them.
“Couldn’t you guys pull off a perfect murder, knowing what you do?”
The pathologists look at each other and grin. There is a long pause before Amador replies, still looking at Escajadillo, “Well...I don’t think you could get away with it twice."
Here's something you might be interested in.
Tijuana coroner's patients cut and sawed open
The body always tells you how it died
Tijuana coroner's patients cut and sawed open
The body always tells you how it died
Many of the names on the chart read simply Desconocido, Unknown, Juan or Juana Doe.
The house of death in Tijuana is the color of dusty bubble gum. Just off the Plaza Club de Leones, with its cathedral-like tower, where Revolucion curves away to the north, SEMEFO, the one-story coroner's office, sits atop a low hill at the end of a sand and cobblestone drive.
I notice that her brain appears fake. I have seen more realistic-looking brains in horror movies.
SEMEFO stands for Servicio Medico Forense, Medical Forensic Service. The dust rises from constant street repairs, from wind that rakes the sand across the cobblestones, and comings and goings of white vans marked D.I.F., with SEMEFO spelled backward beneath the windshield. The vans arrive with a cargo of dead passengers and leave empty.
Technicians greet the drivers at a gate of hurricane fencing and plywood painted gray. The vans back in, the gate is closed, but not before revealing a glimpse of dirty yellow oilcloth or Leatherette curtains that will be pulled aside to admit clientes, as the technicians call them.
The tech presents the left lung in his cupped, gloved palms. Corona points out a black filigree on the organ and pronounces, “Smoker.”
The waiting room is a faded pink, with some of the same charcoal paint used on the gate. Three potted plants seem in need of water. An unframed painting in gaudy golds and muted browns of a galleon at sunset has been punctured at its center.
Doctors Amador and Escajadillo. "There is no such thing as the perfect crime."
The kind of sluggish flies that seem to hover in the dead center of a room in Southern California and Baja in the spring trace lazy spirals and arcs, scattering when someone in the waiting room rises to make an inquiry at the glass partition to the inner office.
Behind me bodies are being removed from the walk-in refrigerator where they are stacked on trays.
The walls at shin level are scuffed and imprinted with small, dirty palm and finger prints. A poster framed under cracked glass has a rose in a clean ashtray with the words Gracias Por No Fumar.
“You will see every type of behavior in this waiting room.”
Manning the desk behind the glass partition is a boy, possibly 20, with a complexion problem, wearing a khaki uniform, a flat-topped haircut, and shiny black-laced shoes beneath frayed pants cuffs. His brass nameplate reads M. Radillo. He answers the phones, makes notes on a clipboard, and enters names in grease pencil on a white plastic wall chart: today’s lineup of clientes.
I see a burn victim that is unrecognizable as either man or woman.
Many of the names on the chart read simply Desconocido, Unknown, Juan or Juana Doe. The chart indicates the time the bodies arrived and were logged in, the date, the day, and their origin, whether it is the street, the prison, or a hospital. “Customers” come routinely from Rosarito and from as far away as Ensenada.
In the waiting room are three women, representing three generations, clearly, of one family. Two children play on the floor, one with a key ring, the other with an empty plastic juice bottle. None of the women are crying or seem visibly upset, though they ration their smiles to the children and the two men who stick their heads into the room every few minutes, between cigarettes. The women do not smile at each other.
“You have a relative here?” Iask.
“Yes,” the young mother nods and says nothing more. Possibly they weren’t close to the relative, but I suspect their lack of apparent grief has more to do with a cultural imperative. Just a few miles north, death always takes place offstage. It is almost always a tragedy and a big goddamned surprise, a dirty trick, unthinkable.
Brain hemorrhage,” says Doctor Corona, a diminutive man in his late 50s or early 60s who wears eyeglasses, a white lab coat, and hair dyed to match his toupee. “This lady has high blood pressure.” He points into the opened skull to a mottling of clotted blood in the top of the left brain hemisphere. “A vascular accident!” he declares with finality.
The woman is a Jane Doe, approximately 45 years of age, with two front teeth of silverish metal that gave her plump carcass the look of a large, flayed rodent.
The handwriting in my notebook is not as shaky as it was several moments ago. When I walked into the room and saw the two corpses (a third one “on deck” on a tray to the left), my reaction was immediate, clear, and probably shameful. I thought. I'm glad it’s them and not me.
The room is rectangular, longer than it is wide, with two chromium tables fitted with slightly sunken drains at their centers. The bodies lie on chrome slats elevated from the pan of the table. Heads are rested on plastic hourglass-shaped blocks. The body on the second table is that of a fat man. His hair is thin, dyed black. He has a mustache. A technician holds a long metal cylinder attached to an amber surgical tube that is in turn connected to a machine: a glass container with several inches of urine-colored fluid at its bottom. The tech has the cylinder or rod inserted into the dead man’s side, just below his rib cage. There is a livid incision just long enough to accommodate the rod. The tech is jiggling the device, working it into the cadaver, causing the dead man to writhe in an undignified way, his thin strands of hair swaying out of place. It is as if the corpse is being tickled, responding with galvanic convulsions of silent mirth he is helpless to stop.
It occurs to me that for some reason the tech is draining the body’s bladder of urine, though I can’t think why this would be done. I am fighting an urge to giggle because it would be inappropriate — all laughter ceases when the doctors, the coroners, enter the autopsy room — and because I am certain that the giggle would escape at a higher pitch than I would like to hear coming from my own throat.
“What is that man doing?” I ask Corona.
“He is preparing the body. There will be no autopsy. Cardiac arrest.” Corona seems uninterested in the case.
The man is being embalmed. I now notice that the level of yellowish fluid in the container is dropping, not rising. He is being pumped full of a formaldehyde-based solution.
This procedure had distracted me while the Jane Doe had been opened from trachea to pubis with a scalpel, revealing an inch or so of fat the color of custard along with her sternum and rib cage. The breast bone was cut by the technician wearing ivory rubber gloves of the type you might wear if you were particularly fastidious while cleaning your bathroom. To cut the chest, the tech uses not a medical instrument, but a garden tool, something with which you would prune a rose bush. The ribs were snapped quickly one after another, the sternum came away in a triangular shape still hinged near the clavicle. The technician bent back the sternum suddenly toward the woman’s face, and it came away in his hand with a snapping noise like someone cracking his knuckles loudly.
I am breathing through my mouth from necessity.
The tech presents the left lung in his cupped, gloved palms. Corona points out a black filigree on the organ and pronounces, “Smoker.” He points with a pen. He does not touch the body; only the technician touches the body. In the next moment the tech is almost up to his elbows in intestines, but not before he has exposed the heart with an abnormally thick layer of bright yellow fat around it: the stuff you trim away from a whole chicken before you roast it.
Corona’s pen points like a divining rod toward what interests him. He takes care not to make contact with the organs, the body, the wetworks, Jane Doe. I am again fighting a slight case of hysteria. I think to myself about Corona, At no time do this dark magician’s hands leave his arms, folks. To cover my discomposure I jot down a note. Thinking of the woman’s approximate age, only three years older than me, I write, “Death seems to age you...or poverty. Maybe poverty and death...” and I lose it. I start to giggle like a schoolgirl catching her first glimpse of a boy’s weenie in the nurses’ office — and it wasn’t what she expected. I cover this immediately by making coughing noises.
“Are you all right?”
“Yes, yes. Sorry.”
After digging through her lower intestines, examining the liver (good, not a drinker or drug user) and kidneys (normal), the tech exposes (scoops out, really) her bladder and uterus; long, straight pubic hairs over a hollow shell where incredibly compact and ingeniously devised reproductive and eliminative soft machinery has been removed. Corona announces, “Now we will look at her brain.”
The tech wrestles the woman’s head back onto the hourglass and places a scalpel beneath her right ear. He makes an incision around the back of the skull and completes it just beneath her left ear. He peels the scalp away like a grape, a banana, a pliant coconut rind. He pulls the front half of it over her face like a stocking cap and reaches for the hacksaw.
Blood, a viscous burgundy, drips slowly onto the gurney.
The tech, whose name is Gustavo, begins to saw in a straight line from her crown toward her ears. My stomach lurches in rhythm with the damp wheezing sound of the blade. Bits of pulverized bone, like sawdust or light snow, fall into the dark pool of blood and onto the surrounding chromium.
I see my reflection in a panel of glass that runs the length of the autopsy room. Beyond the glass I can see the “amphitheater,” several long benches, rising like bleachers, where medical students observe autopsies and hear lectures.
Now Gustavo is sawing in a line that reaches across the woman’s brow. In about a minute, the saw meets the first cut at the top of the ears. Gustavo lifts away the exposed skull, which comes away reluctantly with a sucking sound. He takes a scalpel and cuts at the grey cerebral membrane that clings to the inner skull and brain hemispheres.
Behind me bodies are being removed from the walk-in refrigerator where they are stacked on trays. Many are the bodies of old men, thin, with wispy grey hairs everywhere on their bodies. They all have in common: flattened buttocks and “lividity” or reddish purple mottling of the skin along their backs and buttocks, the undersides of their arms and legs. This is a matter of gravity, the blood settling at the lowest point in the body when it is no longer being circulated.
Turning back to Jane Doe, I notice that her brain appears fake. I have seen more realistic-looking brains in horror movies. This reassures me. Corona points to the left hemisphere and makes his pronouncement about the vascular accident. “She probably eats too much grease.” He nods, satisfied.
Gustavo lifts out the brain. It is slightly larger than his cupped hands, the size of a cantaloupe and flattened at the base. He places the brain into the metal scale suspended over the table and weighs it. It looks to be a little more than a kilogram. A few more measurements are taken, organs weighed. Corona makes notes on the form he has in his clipboard, and the autopsy is completed.
Outside, I draw in lungfuls of air and dust through my mouth and nose. It is delicious, like pepper and salt, orange juice, wine...anything.
That night I dream that Jane Doe is dancing with the embalmed man with the dyed hair. Her right arm is over his left shoulder and poised in rigor as though palsied or in an invisible cast. Her scalp is still peeled over her face, the forward hairs or bangs now a walrus mustache above her two metal rodent teeth. The man shakes with laughter, jiggling like Cab Calloway singing “Reefer Man,” as the couple performs the Forensic Four Step, the Post-Mortem Pavane. In the background Fred Astaire sings, “Heaven, I’m in Heaven...and I hardly feel the ground beneath my feet...” Juana says, “I’d like my face back now. Can I have my face back now?”
Dr. Jesus Ramon Escajadillo, 39, is a handsome man with blue-green eyes and a beard with nascent traces of grey. Today he is wearing a black cowboy hat, striped necktie, and white lab coat. He examines the lineup on the wall board and asks me if I have gotten permission from medical director Dr. Gustavo Salazar to observe an autopsy. I tell him yes and that I’ve already observed one.
“We just don’t want a story about bad doctors in bad conditions doing bad work. That would cause us problems. It would cause me problems, and then that would cause you problems. I know this place doesn’t look good. You could write about the bathroom here alone, never get past that and people would say, ‘Yes, a Third World coroner’s office, it’s terrible.’ We.don’t have the same facilities here as you do in San Diego. But we take our work very seriously. In four months — it has been approved — we will have newer, better facilities here. Construction will begin soon.”
Escajadillo takes his clipboard into the autopsy room and beckons for me to follow. Today, a Monday, the room is filled with corpses. I fight down panic and a rising machaca burrito breakfast as I see a burn victim that is unrecognizable as either man or woman. It is human only in the sense of a charcoal parody done by some grotesque sculptor. Beneath the barbecued head, arm and leg stumps, and torso are lumps of briquets, carbonized calves and feet that are arranged on the cart to suggest where they originally belonged. They could as well be burnt pieces of the building the victim was unearthed from, as far as I can tell.
Next to the burn victim, on the same cart, is the body of a child, maybe three years old. The cadaver is plainly that of a boy with golden hair. One eye is swollen shut and bruised, the color of jacaranda blossoms. “Orbital hematoma,” Escajadillo calls it. Bruises on his legs and arms are apparent, and my first thought is that this kid was beaten to death, but I am wrong.
“No,” Escajadillo says, “he fell, I believe. Five stories from a window.” The child looks angelic. I think of Eric Clapton’s son, then of Studs Lonigan, “Live fast, die young, and leave a good-looking corpse.” Girlish laughter threatens to erupt from my throat again, but it is stifled as if a gimlet were driven into my esophagus by the sight of an infant, possibly six weeks old, his nostrils caked with a white crystalline foam. “What...?" I begin, but Escajadillo shunts me over to the first autopsy at hand. “I don’t know about the infant. We’ll see. First we have this man.”
The customer at table one is “Approximately 25 years of age,” Escajadillo intones into my tape recorder. The body is that of a healthy-looking man in his prime with no apparent evidence of trauma. Black hair and mustache. He is muscular. “According to the information we have from the ministry, he was in a traffic accident. He was riding a motorcycle. He came in at,” he checks his clipboard, “16:30, 4:30 yesterday afternoon. This one,” moving to table two, “is a possible drug overdose. We will run studies to make sure. You see, he is approximately 35 years old.” The man at table two has much grey in his hair, is clean shaven, handsome except that he is as dead as two-toned spats and has foam sluggishly erupting through his nostrils. “Bronchial aspiration,” Escajadillo describes it. “We must find out why.”
A little blood mixes with the foam that had been forced through his nose from his lungs. “He was found on the street," Escajadillo says. The doctor’s guess about overdose seems like a good one. On the cadaver’s right arm is a tattoo of a marijuana leaf. Another tattoo reads P.O.P.E. On the left forehead is dust from the street where he had lain.
With a seamstress’s tape measure, Gustavo, the tech, measures the body’s shoulders, thorax, and abdomen and calls out the measurements in centimeters. Escajadillo writes down the numbers on his form. The body is five meters in height. “The foam tells us, in an indirect way, that the patient died from bronchial aspiration or lung aspiration. But why?"
The tech makes the long incision from the throat to pubic hairs. The lips of the incision peel away from each other with relieved tension, as though his skin had been stretched too tightly over his body. Again a layer of fat, but much less of it than on the Jane Doe. Escajadillo peers into the trachea, pointing with his pen. Gustavo leans over and with his scalpel opens the trachea farther. More foam and more blood. His scalpel flicks a droplet of blood onto the coroner’s white lab coat. The doctor backs away saying, “Hey! Hey!” and then laughs. Gustavo laughs and apologizes.
“From the tattoos, the maguey plant? No, a marijuana plant with the name Toni above it, and this one,” points to the second tattoo on the lower right arm, “we might assume he is a drug user whose name is Toni or Pope” (po-pay). “We will look in his liver, his stomach, heart, and kidneys, and we will run some tests.” Escajadillo makes a notation that the “patient” has two tattoos on his left side. They are in fact on his right side, but I do not correct him.
“I can’t see any sign of trauma or violence. There is an abrasion on the knee that occurred eight to ten days ago.” Looking into the mouth. “Teeth are incomplete.” He writes this down. “Male, regular complexion, eyes brown, forehead wide, his mouth is regular, teeth incomplete, no mustache. Between 35 and 38 years old. Chin is square, regular ears. Now sometimes you cannot see any signs of trauma on the outside, but will discover a hematoma inside. This is clean, no trauma. Internal hematoma looks violet in color with a little bit of blood around. Let’s have a look the heart.”
Gustavo is cutting away at the protective tissue around the heart. A pale, bloody fluid escapes. “This liquid is normal. We can have as much as 16 milliliters of liquid around the pericardium, so he is normal here. Not too much fat around the heart, but you can see here,” he points with his pen, “you can see here in this small coronary artery, signs of arteriosclerosis.” He is pointing to what looks like a pinprick along the surface of the heart. I would never have seen it. “It means his levels of cholesterol were probably high, but there are no signs of a heart attack at least in the anterior compartments. Now we'll have a look at the posterior compartments...” Gustavo flips the heart in his hands, exposing the B side. “Posterior compartment is clean. No signs of recent heart attack. Now we have to look at the lungs.
“Now this man is a smoker, this is called anthracosis.” Later, looking up the word, I see that it is derived from anthracite and literally means the condition derived from inhaling coal dust. “You see this, these spots of blood? We call these Tardieu spots in forensics. These spots tell us that this man had severe hypoxia [lack of oxygen] before death, which is compatible with what we see there with the foam. We are pressing the lungs, you see?” Indeed Gustavo is squeezing the purple-and-black mottled organs like bellows. More bloody foam erupts from the patient’s nostrils.
On the next table, the cadaver of the 25-year-old has been opened, his skull peeled away. The smell is much worse from this corpse because of the amount of time transpired between death and refrigeration. The doctor in charge of that case is Dr. Amador. I ask Escajadillo if the smell ever gets to him.
“If the body has been dead for weeks, it can get bad. This isn’t bad. This man,” indicating the bronchially aspirated man, “has been dead less than 48 hours.”
“So you get used to it?”
“Yes,” he shrugs. I don’t believe him. I can’t imagine getting used to it, but no one else in the room seems uncomfortable. “Look here,” pointing to the opened throat on the body, Toni or Pope. “The trachea is full of secretions. You see the foam coming out? Now let’s check the liver. It seems fine. This is the spleen. Fine. Now here is the stomach... you can see here several things,” but he is not pointing to the stomach but to the small lower intestines that Gustavo presents by the handful like long, thin balloons or pale sausages. Escajadillo assesses the organs with what appear to be almost cursory glances, but he knows what he is looking for. “This man has intestinal bleeding from the small bowel. You can see the discoloration (a dark section of tubing] in this section of the lumen. There is a gastrointestinal problem with this man.”
Examining the pancreas, the doctor seems satisfied. Behind me. Dr. Amador’s tech has started sawing the skull of the motorcycle accident victim. The sound sends my stomach into fitful lurches again. To shift my focus, I ask Escajadillo if he could venture a guess at this point as to the probable cause of death of his “patient.” He smiles and shakes his head, “We don’t guess,” he says.
Gustavo exposes the kidneys. The left one seems normal, but the right one is at least twice the size of the left. “We call this hydronephrosis.” The examiner instructs Gustavo to open the stomach. Gustavo takes his scalpel and punctures the bladder, tears it, the way you might open a bag of potato chips with a letter opener. I peer inside at a green fluid. “Bile?” I ask wrinkling my nose.
“Salsa verde.” Escajadillo smiles. “It went up to his throat, to his trachea, causing bronchial aspiration. There is bleeding and edema in the small bowel. Several things may have happened. He may have had intestinal infection which caused him to vomit, which in turn caused the aspiration. But a lot of us have infection, throw up, and cough, but we do not die. So why did he die? Besides the intestinal problem, he has the hydronephrosis of the kidney. Two pathologies we can see now this patient had. We have to be sure he did not also ingest alcohol. We will run tests, primarily blood tests, but we will run a sample from the stomach for drugs or infection. Mostly we must quantify the blood alcohol level and test for certain drugs. After this lab report, we will be able to determine what is acceptable as the cause of death. But we have an idea now.”
“Food poisoning?” I ask.
He nods, “That is possible, that is why we are going to run the contents of the stomach. Make a culture. It takes about three or four days. I am going to make my preliminary report that the cause of death was bronchial aspiration. I will sustain that pending the results from the lab tests. You see? We have to wait.”
A forensic chemist comes every day to take away samples to be tested. He is paid by the state, a member of the forensic department, referred to as the ministry, the umbrella office of the state police.
Again with the saw, Toni’s brain is opened. “We have to look for trauma or congestion,” Escajadillo says. “We have to be sure that the brain has not been involved in violence...trauma. There is some cephalic congestion, you see,” In fact, I do not see what the coroner is seeing. Possibly it is a purplish clotting of blood to the left of the left hemisphere. “Probably because of the hypoxia.” We wait while Gustavo removes the section of skull. I ask why no one is making jokes the way you see medical examiners doing in American movies. “Well, sometimes, “ the doctor says, “but we do not joke at the expense of the body. Sometimes we will joke about the situation in the examining room or events that surrounded the death, but in general we try to be respectful.
“You see our electrical saw is not working,” he points to a white circular saw sitting off to one side.
“The blade is not sharp enough. We’re waiting for new blades. The hacksaw is good, but we have to improvise often, like the shears. Whatever works is fine. We’re not dealing with living tissue.
“We would like to have a little more good equipment, of course. That would help. We even need a new pair of scissors. If we could change the equipment every year, that would be great for us, but sometimes it’s just not possible. We’re working on it. You see the congestion here. We need more space.”
The word “congestion” seems to remind Escajadillo of the job at hand. He points to the brain again with his Bic Fine Point. “This is compatible with all the signs we saw in this body. We can see some periosteal seams, another sign of hypoxia. Now we will take out the brain, see if there is any sign of skull fracture or hemorrhage in the ventricular system of the brain. We want to remove the dura, the membrane, so we can see the bone and any irregular lines, like cracks. Here we can see the anterior compartment, the olfactory nerve, the roof of the ear, the fifth cranial nerve, the third cranial, the hypoglossal nerve, the optic chiasma...." As the litany is intoned, Gustavo draws blood from the empty brain pan with a hypodermic the size of a turkey baster. “Here is the seventh cranial nerve which moves the face. The eighth governs hearing and vestibular function...not to be dizzy, you see?”
Again Gustavo accidentally spatters a little blood on the coroner. Escajadillo laughs and in mock outrage says, “Hey hey hey hey hey!”
He introduces me to Dr. Julio Javier Amador Barragan, who is conducting the autopsy on the hapless motorcyclist. Amador is 32, with a round, pleasant face. He wears a blue smock instead of a white lab coat.
“A motorcycle accident,” Amador begins. “He has trauma to the brain and the thorax. Brain hemorrhage and lung hemorrhage. We will examine the abdominal wall and cavity.”
Since Amador has established two separate causes of death, why look further?
“Although he has damage to other organs, we know that the damage to the brain is not compatible with life. He might have survived the trauma to the thorax. He was a smoker, and this discoloration of the lungs indicates that his lungs were attached to the ribs. This individual had chronic lung disease. We cannot establish at this point if he was exposed to tuberculosis or some other form of disease.”
He wasn’t wearing a helmet?
“It is not established in the reports we have, but I can assure you it is uncommon for these guys to wear helmets. He was not wearing a helmet. We don’t know his name. The reason we keep looking beyond the possible or probable causes of death is that there may yet be others. Even something you would think as obvious like a gunshot wound can be so small you cannot sec it clearly. There have been many cases where an individual has been killed and then has an apparent car accident. You have to look for further causes. We are obligated to the police department, the justice system. This is one reason, simple thoroughness is another."
I venture my theory that the Juan Doe had a coughing fit while riding his motorcycle and crashed into something.
“We cannot determine that. We would need a crystal ball to establish he was coughing before he died. We can establish, because of the fibrosis and the lung’s attachment to the ribs, that he had a problem. Whether the problem had anything to do with the accident, we can’t say.”
“Sounds like his number was just up,” I say, but Amador looks puzzled, as if he doesn’t know what that means. Certainly I don’t either, so I say nothing more.
At this point Escajadillo calls my attention back to the previous autopsy. “We are weighing the kidneys,” he announces as if this is something he wants noted. “The one on the right side weighs 200 grams. The one on the left is 150 grams. We have trimmed all the fat tissue away. You see the difference?”
Escajadillo moves to the charred corpse and signals me. “This is Doctor Quiroz.” He indicates a pretty and full-figured woman in a lab coat. “This is her case. Looks like 100 percent burns, say 98, we still have some tissue at the right breast. Usually this happens at home. Maybe she was living in not very good conditions and was trying to get warmer at night. Maybe she tried to burn something for heat, and the whole house, whoosh! This is more common in the winter, but there could be other causes. Some criminals when they want to get rid of someone and they shoot or stab someone, they will burn the body. They think by doing this we won’t find out what really happened. In each burn victim — we study them, take X rays, everything.”
In a body this badly burned could the pathologists find gunshot wounds or stab wounds?
“Yes. We will find it. The general rule is...”
Here Amador interjects happily, “The body always tells you how it died,” and smiles at Escajadillo.
“Yes. The body is always trying to get your attention. You just have to be sensitive to the correct diagnosis.”
What percentage of bodies that come in are victims of violence?
“We have statistics from last year [1992]. The main reason of death is trauma, mostly related to accidents, number two is heart attack, the third leading cause of death is due to firearms, the fourth is bronchial aspiration, the fifth is death related to the use of knives. We call those arma blanca or white-arm killings. The rest is gastrointestinal, like cirrhosis, liver problems. Now with the summer we will have a lot of drunk people, alcohol-related deaths.”
What happens when Americans come down here and die? “By law we have to do the autopsy here. We can’t send the body to the United States for an autopsy because the Mexican authorities have to be informed by the same system here in Mexico as to what was the cause of death. The explanation for this is simple if you think about it.”
Amador then points out to me that his motorcycle rider has traumatized kidneys, though I cannot detect the damaged tissue or distinguish it from healthy tissue. He will also order blood tests and stomach cultures.
Escajadillo moves to the child who had fallen out of the window. “See, he fell from a fifth floor, but he survived a little bit afterward because we see medical sutures.” He points to stitches on the child’s neck. “And we see here an injection mark, a puncture at his ankle where he was given saline or blood or something, some IV fluids. I think he was two or two and a half.”
'The infant on table four, possibly a month or two old, is several feet away, the province of Dr. Quiroz. Escajadillo looks at the tiny boy and points out the crystalized foam around its nostrils. “Bronchial aspiration again.” He points to yellow-green stains around the child’s bowels and genitals and says, “This liquid staining makes me think a respiratory or gastrointestinal dysfunction. We will not do an autopsy, the public minister does not require it. There is no question of any crime related to the death." Escajadillo’s dismissal of an autopsy seems to be borne out of a reluctance to desecrate the body of an infant, possibly weighing what forensic science would learn against the abhorrence of mutilating something otherwise perfect. I am speculating, but I sensed Dr. E. did not want to dwell on this case.
“Is there any indication,” I ask, “that the death might have been prevented?”
“It is very hard to say. Sometimes when the parents are concerned about a common cold, the child may die anyway. Sometimes the parents are negligent, a lack of concern, but this is impossible to say in a case like this. So what is the point?”
The coroners dismiss me as the autopsies are completed. I wait in the driveway sucking lungfuls of air as two well-dressed men in their 30s emerge from the medical director’s office. They are reporters from El Mexicano, the Tijuana daily newspaper. They are, they tell me, following up a story on the likely murder of two prisoners by federale officers in the T.J. pen, the Casa Blanca.
“One of the guys has a fractured skull, the other one, we don’t know or they won’t tell us. They said come back tomorrow or the next day.” This was something I had been told for days while waiting to get inside SEMEFO. “It is a very dark business. Maybe you can find out something.”
Indeed, I ask Amador and Escajadillo when they emerge from the autopsy room around 11:30 a.m. They must both resume their private practice for the rest of the day; Escajadillo as an ear, nose, and throat physician and Amador as a general practitioner.
“Yes, one of the prisoners had a fractured skull,” says Dr. E. “The other one, I don’t know. It’s not our case, and I don’t know if we’re supposed to say anything.” He looks at Amador, who shakes his head.
“No, says Amador, we can’t say. You will have to talk with Dr. Salazar.”
I ask Amador about the unhappy people in the lobby.
Relatives of the deceased? “Very often. Sometimes people are just looking for someone who is missing. This is the last place you look because it is the last place you want to look, of course. Some are here to be certified for wounds or injuries that occur in violent situations. We don’t treat them, but we look at them and certify that they have such-and-such lacerations, contusions, or abrasions, how long it will likely take to heal, and things like that. We sign the papers and they go back to the D.A., who gives the certification to the judge. We work with people who are alive too.”
Escajadillo adds, “You will see every type of behavior in this waiting room.”
Jesus Ram6n Escajadillo has been in forensics for seven years and claims, “I would do it even if I were not being paid. It is like my hobby in many ways. It makes me a better doctor, and I am always fascinated. No one does this just for the money. I can speak for 100 percent of the doctors, I believe. Forensic pathologists in the United States make many times what we are paid to do this one week out of every month. Well, we end up working more than that with court time and everything.”
Escajadillo considers himself a medical scholar, his ENT practice enables him to “survive,” and he adds “something more than $12,000 a year” to his income by his work at SEMEFO. He studied in Mexico City and then served a fellowship in Holland for two years studying thoracic surgery. He trained for another two years in Tijuana as a forensic doctor.
Why would anyone seek out this work? How can you get used to this, much less love it?
“You have to have a special interest, a predisposition. I can’t explain it. Look, I have been here for several years and sometimes...mainly, mainly with the kids...I can’t understand...it’s very hard for me to see...people who didn’t have any reason to die. People crossing the street and a drunk kills them, that’s hard. But children especially...children. It’s hard when you deal with a body who has been decomposing for a long time. Not easy. I’ll tell you. But I feel like I’m helping the community. I’m part of the community, and we are, all of us, moving into the next century and I feel a part of it.”
Amador’s interest is in “enforcing the law. This gives me an opportunity to learn how much violence there is in my city and that something is being done about it or maybe nothing is being done about it. If nothing is being done in a particular case, it is not because of me. We see cases that were misdiagnosed, and it is our job to say so, even if this does not make us popular with the medical community here. Sometimes we are considered, by other doctors here...ahh...”
“Pains in the ass?” I suggest.
Amador smiles. Escajadillo illustrates the necessity for the Tijuana Forensic Office’s services with a case in point. “There was a female patient — excuse me for saying patient, it is a habit — she was the mother-in-law of a guy who lived here in Tijuana, though she lived in, I think, Chula Vista or National City. The mother-in-law didn’t like the son-in-law. She had a very prosperous business. Her son-in-law was working with her and he got fed.up with her behavior. He tried to make the perfect crime of her.
“Some of the neighbors of the woman heard an argument with her and the son-in-law that ended abruptly. He stabbed her about 250 times. He tried to clean up all the blood and take the body to Tijuana. He put her in the trunk and went to la presa, the reservoir. He put gasoline and kerosene in the car, and everything was completely burned. The police sent us small burnt pieces of this lady. You saw that burned lady this morning? That was nothing. Anyway, we found something was very much wrong with this burn victim; wounds that were not compatible with a car accident and fire. We found lesions and trauma to the bone fragments. We told the police here, ‘This was a crime.’ So they contacted the SDPD liaison guy and found out that they were missing a body in what was obviously a homicide of a brutal nature. We gave them the autopsy report, and they put this guy together with the victim.” Did they arrest the guy?
Dr. E. looks at Dr. A. quizzically. “Yeah, I think they got him. We handed them everything.”
Dr. A. says. “I think they made the arrest.”
“You see?” Escajadillo says. “We need better communication with the other side. We should have meetings once a month with the forensic guys in San Diego and theTJ guys. We share the same problems, the same crimes, the same criminals. Half the time our victims are related to somebody with a file on the other side.”
Amador leans forward, “You see, his story tells you. There is no such thing as the perfect crime. The body always tells you how it died.”
“No such thing as the perfect crime?” I ask both of them.
“Couldn’t you guys pull off a perfect murder, knowing what you do?”
The pathologists look at each other and grin. There is a long pause before Amador replies, still looking at Escajadillo, “Well...I don’t think you could get away with it twice."
Comments