{kind=link}
Here's something you might be interested in.
Ask a Hipster — Advice you didn't know you needed
Big Screen — Movie commentary
Blurt — Music's inside track
Booze News — San Diego spirits
Classical Music — Immortal beauty
Classifieds — Free and easy
Close to Home — What it’s like on the street where you live
Cover Stories — Front-page features
Drinks All Around — Bartenders' drink recipes
Excerpts — Literary and spiritual excerpts
Feast! — Food & drink reviews
Feature Stories — Local news & stories
Fishing Report — What’s getting hooked from ship and shore
From the Archives — Spotlight on the past
Golden Dreams — Talk of the town
The Gonzo Report — Making the musical scene, or at least reporting from it
Letters — Our inbox
Movies@Home — Local movie buffs share favorites
Movie Reviews — Our critics' picks and pans
Musician Interviews — Up close with local artists
Neighborhood News from Stringers — Hyperlocal news
News Ticker — News & politics
Obermeyer — San Diego politics illustrated
Outdoors — Weekly changes in flora and fauna
Overheard in San Diego — Eavesdropping illustrated
Poetry — The old and the new
Reader Travel — Travel section built by travelers
Reading — The hunt for intellectuals
Roam-O-Rama — SoCal's best hiking/biking trails
San Diego Beer — Inside San Diego suds
SD on the QT — Almost factual news
Sheep and Goats — Places of worship
Special Issues — The best of
Street Style — San Diego streets have style
Surf Diego — Real stories from those braving the waves
Theater — On stage in San Diego this week
Tin Fork — Silver spoon alternative
Under the Radar — Matt Potter's undercover work
Unforgettable — Long-ago San Diego
Unreal Estate — San Diego's priciest pads
Your Week — Daily event picks
What San Diegans do now when knee cartilage tears
The rise and falls of the amateur athlete
Arthroscopic surgery engenders professional jealousy among some colleagues.
Flexibility and strength. Range of motion. These are the keys to avoiding any athletic injury, or so claims Phil Tyne. Tyne owns an athletic club in downtown San Diego and he is also the conditioning coach for the San Diego Chargers; you have to believe he knows something about athletic injuries.

“It’s weekend and amateur athletes who get hurt the most."
Professional athletes get injured often enough these days, he concedes, but they would get injured a lot more often if they weren’t in excellent physical condition. “Actually, pro athletes have an advantage; they can work at staying in shape seven days a week,” Tyne says. “It’s weekend and amateur athletes who get hurt the most. You leave your office on Friday evening and the next day you’re out running or playing racquetball or soccer. And in the heat of competition you maybe have to stretch further than you ever have in your life. You overdo it, and suddenly you're in a situation you can't get your body out of.’’
Phil Tyne: “You can’t prevent injuries, but you can increase the odds of not having them.”
Take Joe, for example, one of Tyne’s current customers at the club. Joe is thirty-five years old. six feet, two inches tall, and just a shade over 200 pounds. He has the dark hair and quick, sarcastic wit you often associate with people from the East Coast, and as a matter of fact that’s where he’s from — Syracuse, New York.
Removing bits of torn knee cartilage remains one of the commonest and most practical applications for the new surgical technique.
Joe (not his real name) used to play a little football in high school and college, but ever since he passed the bar exam and moved out to San Diego he hasn’t had much time to stay in shape.
Byron Wildermuth: “We go through a lot of ice here.”
You might have seen his law office in Hillcrest — one of those converted Victorian houses with beveled glass windows, carpets an inch thick, and a lot of expensive antique furniture.
Well, three months ago Joe went skiing for the first time in two years and got his body into a situation he couldn’t get it out of. Technically, of course, he did get out of it, but not before ripping apart the cartilage in his right knee. Now, after surgery, a short period of rest, and six or seven weeks of rehabilitation therapy, he’s trying to work himself into good physical condition at Tyne’s club.
“We’re not doctors and we’re not physical therapists,” Tyne tells potential customers like Joe who have had serious injuries. “We don’t cure anybody in here. But we’ll work as closely with your previous therapy as we can, and we’ll strengthen the affected area as much as possible. The better shape you’re in, the less likely it is you’ll re-injure yourself.” So Joe comes down to Tyne’s club once a week and strains and puffs along with overweight businessmen and housewives, fine-looking college athletes (both women and men), and a couple of people recuperating from injuries such as his own.
It costs him additional time and money on top of the three months and thousands of dollars he’s already spent on surgery and rehabilitation therapy, but if you bring up that subject, Joe will just laugh and say he’s only doing his part. The American public’s modern penchant for physical recreation has led to a burgeoning number of athletic injuries, and this in turn has led to increasing work for orthopedic surgeons, new surgical techniques, special therapy clinics with even more specialized equipment, and even experts like Tyne who concentrate just on trying to prevent injuries. Only ten or fifteen years ago Joe would have had an operation and afterward would have been more or less on his own. “Oh, the doctors might have told me to wait six weeks and then give my knee some exercise, but most of them wouldn’t have been able to say exactly what I should do,” Joe told me one evening after his workout at Tyne’s club. “The way I figure it, I was probably lucky to injure myself in 1981.”
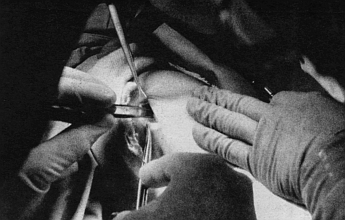
The scissors that clipped Joe’s torn cartilage and removed it from inside his knee are the size and shape of a large screwdriver. By pressing a lever on the handle, tiny blades on the end of the long, needlelike point can be opened and closed almost effortlessly. I saw the scissors not long ago in the office of Dr. Rory Bergen, one of several orthopedic surgeons in San Diego with extensive experience in athletic injuries. Bergen pulled the instrument from a box that was stored behind his desk and said with a mischievous smile, “To stay current in this business you really have to be something of a gadgeteer.” Then he deftly snipped two small V-shaped notches in an invoice on his desk to show me how sharp the scissors are.
“There are a lot more people coming in to see orthopedic surgeons these days,” Bergen told me. “Athletic injuries are on the increase because of the population increase in general, and also because of the fitness renaissance. But one of the biggest reasons has been the increasing involvement of women in athletics. In a way, they have sort of doubled the population,” or at least doubled the number of patients for orthopedic surgeons.
Most of the patients Bergen sees have serious injuries — torn ligaments or cartilage, or badly broken bones. To correct these problems he employs arthroscopic surgery, a new technique which seems to have clear-cut advantages over the old operating methods. But it is a technique which also engenders professional jealousy among some colleagues, and so Bergen requested that his true name not be used in this article (it isn’t). Some doctors who still use the old techniques feel threatened by the new ones, he said, and part of the reason could be the considerable investment of time (for learning) and cash (about $15,000 worth of equipment) that arthroscopic surgery requires. If Bergen’s true name were to appear here, some doctors might accuse him of being on an ego trip or advertising “his” methods through the media. “And in a way they’d be right, because a lot of people read your paper, and it would amount to an inadvertent advertisement,” Bergen told me. “And frankly, I don’t want that at all. I’m always behind schedule; I’ve got more patients than I want already. But on the other hand, I think all doctors will be using these techniques in five years, and I think the public has a right to know about them.”
Arthroscopic surgery employs the kind of specialized, sophisticated instruments that laypersons are amazed to learn even exist. These instruments have enabled surgeons to reconstruct torn ankle, knee, and shoulder ligaments from a patient’s tendons, and also, in some cases, to sew ligaments together. Bergen says that someday soon surgeons using arthroscopic surgery might even be able to sew torn cartilage back together. For the time being, however, removing bits of torn knee cartilage remains one of the commonest and most practical applications for the new surgical technique.
The cartilage in your knee is a rubbery tissue that lubricates and cushions the area where the femur (upper leg) rests upon the tibia (lower leg). According to Bergen, the cartilage distributes the weight of the upper body in a remarkably efficient way. “Studies have shown that the pressure goes up fantastically high without any cartilage in there,” he says. But because most cartilage has no blood vessels in it, and thus doesn’t receive nutrients, it cannot heal when damaged; and torn cartilage, if left in the knee, can cause the joint to buckle, lock up, and otherwise malfunction.
Until recently, Bergen explains, if X rays disclosed that you had torn your knee cartilage, you would have gone to a hospital and had the entire cartilage removed through a two-inch incision in your knee. “But a number of us became increasingly dissatisfied with that, because long-term studies showed that with full removal of the cartilage, fifteen or twenty years down the line a high percentage of patients would complain of pain and restricted motion in their injured knees. But on the other hand, it’s difficult to remove only a part of the cartilage with a skin-incision-type operation.”
According to Bergen, it wasn’t until 1974 that an instrument was perfected which enabled surgeons to look directly inside of knees and other joints without cutting them open. Called an arthroscope, it looks a little like a periscope with the eyepiece attached to the upper part. The bottom part is a pointed rod with a light and a magnifying lens at the end, and it can be inserted directly into a joint. The surgeon peers through the eyepiece and can examine the injured area virtually at his leisure. (“Unlike some joints, the knee has a lot of space inside it,” Bergen told me when I asked. “It’s like a little room in there.”)
About the same time the arthroscope was invented, microsurgical instruments were developed which allowed surgeons to perform much finer and more delicate operations than before. Orthopedic surgeons soon became interested in utilizing these instruments in combination with the arthroscope for a variety of operations, and arthroscopic surgery was born. Bergen says that much of the modem surgical technique for removing only part of a knee cartilage was pioneered by Dr. Richard O’Connor of Inglewood, California, and adds with a note of awe in his voice that O’Connor died of cancer recently “after having done at least 2900 knees.”
When Joe first showed up at Bergen’s office, he complained that his knee had been giving him problems ever since he had taken a spill while skiing a few weeks earlier. It didn’t really hurt that much, he said, it just didn’t seem to be working right. Bergen asked him to describe the accident, and the full story, as Joe described it to me later, went like this:
Right after Christmas last year he and his wife Sherry drove up to Mammoth for three days of skiing. It had been a dry winter so far, and they could see rocks here and there sticking up out of a shallow, twenty-inch base of snow. After the first morning, Sherry decided to catch up on her reading at the condominium they’d rented, but that afternoon Joe took the lift up to the Cornice. He’d never been up to the Cornice, a dangerously steep slope for experienced skiers, but it was the highest slope at Mammoth, and Joe reasoned that the higher he went the more snow he’d find. He was right, but there were still a few rocks dotting the snow as he pushed off down the run. The first part of the Cornice is a nearly vertical drop, and for thirty feet or more Joe’s skis never even touched ground. After that he was rocketing down the slope, faster than he’d ever gone before, the wind stinging his nose and cheeks like a caustic chemical. He turned quickly left, then right, and was leaning into the hill to turn left again when his skis hit a rock and he started to slide. Instead of falling, he straightened up and tried to regain his balance, a trick he’d employed with much success on smaller slopes. This time, though, the edge of his right ski dug into the snow, the binding didn’t release, and for one awful instant Joe’s leg was anchored to the hill while the rest of his body twisted up into the air. He felt a hot, searing pain in his knee, and then he was airborne. “All I could see was my skis and blue sky. I knew I was going to hit ground soon and that I better do something about it. But, oh mother, the pain in my knee. . . .”
By the time Joe had skidded to a halt, the pain had virtually subsided. He even got up and finished the run. His knee felt weak, but not as if he had seriously damaged anything. Still, he was a little shaken up, and he called it a day and made his way back to Sherry and the condo.
The next morning his knee was swollen the size of a cantaloupe. Sherry was appalled, and all the way back to San Diego she kept telling Joe he must have done something really bad to it, that he’d better go see a doctor right away. But Joe’s the kind of guy who’s always had, well, not exactly a fear of doctors, but a strong dislike. He’d hurt himself a few times playing football, but he’d never gone to a doctor then and things had always turned out fine. So he held off, and for a few weeks his knee actually seemed to be getting better. The swelling went away, and even though he couldn’t put much weight on it he could get around with the help of a cane. But one afternoon he was getting out of a car in front of his office and his knee just seemed to freeze up. No matter what he did he couldn’t get it to straighten out, and finally he decided he’d pay a visit to someone like Bergen.
Bergen could see that Joe’s right leg was already beginning to grow thin from lack of use. When the X rays showed no broken bones, bone chips, or anything else in the knee, he asked a few more questions and ran a few more tests, and then told Joe that it looked like a torn cartilage. Bergen said he would schedule an arthroscopy for the following week and could remove the torn part of the cartilage then. Joe just nodded and went home to bite his nails.
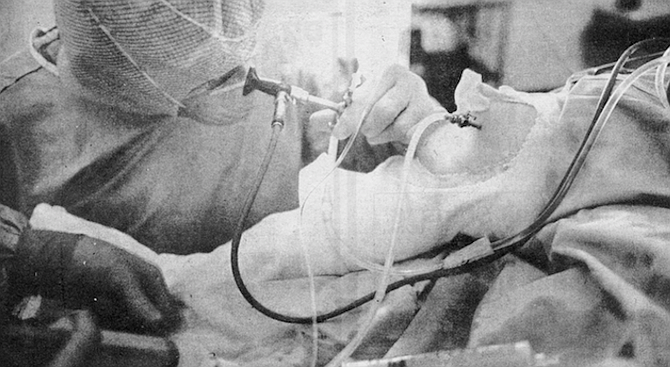
The operation to remove Joe’s torn cartilage went as smoothly as it could. Joe showed up at the hospital at nine in the morning and was out cold by ten. Bergen shaved the injured right knee with a little lawnmower-like device that cuts hair and sucks it up through a vacuum hose, and then used a syringe to inject Joe’s knee with saline solution. Soon the joint was swollen to twice its normal size — a painful but necessary step that gives the surgeon more room to work and is the main reason for keeping the patient unconscious throughout the operation. After that Bergen put in the arthroscope.
“This surgery is designed to preserve as much of the cartilage as possible,” Bergen explains. “Technically, it’s super-difficult for the surgeon. It’s tedious. It takes a long time to learn, and you have to be patient.” Peering through the arthroscope, the surgeon searches the inside of the knee for the torn piece of cartilage. Once he locates it he punches two more holes in the skin of the patient’s knee, one for the blunt-nosed “hook” and one for scissors. Staring through the arthroscope the entire time, he maneuvers the hook under the torn cartilage and lifts it up. “Then,” says Bergen, “you reach the scissors in through the other hole, snip off the torn part, and extract that baby right through the skin.” On the average, the operation takes Bergen about forty minutes, and at least once he has affixed a video camera to the arthroscope and maneuvered his instruments while watching them on closed-circuit TV. “Aside from joint implants, it’s one of the most exciting things that’s happened in orthopedics recently,” he says with genuine eagerness.
Including the use of the hospital facility for half a day, the anesthesiologist’s fee, and the surgeon’s fee, the operation costs in the neighborhood of $2000. But Bergen figures that’s still cheaper than the old operation, which requires a hospital stay of two or three days as well as a surgeon’s fee and other costs. In addition, a patient who has had his entire cartilage removed is usually on crutches for one week and is unable to exert himself physically for four to six weeks. But the patient who undergoes a partial cartilage removal, Bergen claims, “winds up with three stab wounds instead of an incision. Usually he can walk away from the operation once the anesthetic wears off. He can go to work the next day.
“The disadvantage is that you might leave cartilage behind that could tear again, but that doesn’t seem to be happening,” he continues. “We don’t really know what the long-term results will be, because the techniques just haven’t been around that long. But to me there’s no question that the results will be comparable to or better than the old operation.”
A week after his operation Joe was back in Bergen’s office for a checkup, thanking him and saying that his knee felt a lot better. But because Joe had waited so long to have it operated on, Bergen advised him to see a physical therapist to build up his atrophied leg muscles. He recommended a place called the Sports Injury Clinic, which specializes in rehabilitating athletic injuries. “The most important thing for you to do after a knee injury,” Bergen emphasized as Joe was leaving his office that evening, “is to get your muscles rehabilitated.”
Joe recalls that when Bergen first mentioned the Sports Injury Clinic, his first thought was: “You’re kidding — a clinic just for sports injuries?” He concluded it must be a place where local college and professional athletes go to recuperate from their battle wounds, and he joked with Sherry about sitting on an exercycle next to Louie Kelcher or Ozzie Smith, bantering about bygone Super Bowls or World Series. It didn’t turn out that way.
The Sports Injury Clinic is housed in a new shopping center complex on Aero Drive, just south of Montgomery Field. There is a Japanese restaurant on one side and a film processing shop on the other. You enter through double glass doors and find yourself in a wide, open room furnished in a way that might be described as “pleasantly modern.” Everything that isn’t glass or natural wood seems to be gleaming chrome or vinyl. The walls are sparkling white and the rug is an earthy brown.
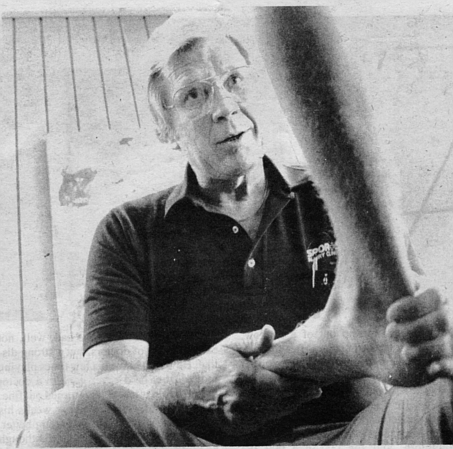
The clinic was founded three and a half years ago by Dr. Robert Moore, a teacher and trainer at San Diego State University, and Ric McDonald and Dick Dent, the Chargers’ and Padres’ trainers, respectively. Its current director, however, is Byron Wildermuth, a tall, confident man of forty-six with clear blue eyes and longish white hair that lends an air of distinction to his overall appearance. In addition to being the clinic’s director, Wildermuth (his real name) is a registered physical therapist, and personally supervises the rehabilitation programs for some of the clinic’s patients. “A clinic like this might seem like a new phenomenon, but it really isn’t,” he says. “Pro athletic teams have always had their high-priced doctors, trainers, and exercise equipment. We bring that expertise to the athlete who didn’t have access to this kind of thing before.” A few of the clinic’s patients are professional golfers and tennis players who don’t have access to team trainers, and in the past a few superstar athletes like Bill Walton and Willie Stargell have also used the facility. “But most of the patients here,” Wildermuth says, “are amateur and recreational athletes — the office-worker-runner-skier type. Most of them have some sort of mechanical problem with a joint — knees are the most common, then shoulders and ankles — but we treat sprains, tendonitis, everything down to tennis elbow.”
In addition to Dent, McDonald, and Moore, who work at the clinic part-time, the staff at the Sports Injury Clinic consists of Wildermuth and several certified athletic trainers. Athletic trainers need to pass a standard test to be certified at their profession, and some begin to prepare for that test as undergraduates at San Diego State, where a growing athletic medicine program includes classes in human physiology, corrective and orthopedic physical education, and weight training, among others. In order to gain a trainer’s certificate the students must also serve two years as an intern to a certified athletic trainer, a requirement most do not fulfill until after they’ve obtained their Bachelor’s degree. A physical therapist like Wildermuth needs to pass a certification test, too, and as an undergraduate takes classes similar to those taken by aspiring trainers. But his education includes less on-the-field experience in such specialties as first aid and taping, and his required internship with a registered physical therapist is only five months.
I accompanied Joe the first afternoon he went to the Sports Injury Clinic. After filling out the prescribed forms and handing over a “surgical report” prepared by Bergen, he chatted with Wildermuth about what type of surgery he had had, and whether or not he was still having any pain in his knee. Then Wildermuth directed him to the men’s dressing room. Joe returned a few minutes later wearing only athletic shorts and a T-shirt, and Wildermuth measured both of his knees, just above the kneecap. Joe seemed genuinely upset when he learned how much his injured leg had atrophied since his skiing accident; it was nearly two inches thinner than his good one. In fact it was a pasty, scrawny-looking thing, more like a child's arm than the leg of a grown man. The three small scars from his operation glistened on his knee like some sort of giant cobra bite.
Wildermuth next led Joe over to a row of vinyl-covered tables, a few of which were already occupied by other patients. Some of the patients were women dressed in dark-colored dancing tights with running shorts pulled on over them, and others were men dressed in shorts and T-shirts like Joe. Wildermuth indicated one of the empty tables, and Joe hoisted himself up on it and gingerly stretched out his right leg. Then Wildermuth brought over a towel filled with ice and proceeded to wrap Joe’s knee with it, fastening it in place with an elastic bandage. “We go through a lot of ice here,” Wildermuth explained as he worked. “About 1000 pounds a day. It’s called cryotherapy, and it’s really just an adjunct to our regular therapy. Ice increases the circulation and lessens fatigue.
It controls swelling, decreases spasms, and has a slight numbing effect that allows us to work you relatively pain-free.” When Joe asked if there were any injuries that heat was good for — as in Jacuzzis or hot whirlpools, for instance — Wildermuth shrugged. “I suppose so,” he said. “But we feel ice is better. You always put ice on an injury for the first forty-eight hours. Some people say you should apply heat after that, but we get better results with ice.”
When he had finished wrapping Joe’s knee, Wildermuth set a small plastic timer for fifteen minutes and then sat down in a chair next to the table. As the timer ticked away he told Joe that the other patients at the clinic had come in on their doctors’ recommendations. “We work on doctors’ referrals only,” he explained. “It’s like a prescription for drugs — your doctor gives us a diagnosis and a broad prescription for rehabilitation, and we take care of the specifics.” Treatment can vary from one day to eight weeks, he added, depending on the injury, and is virtually the same for an amateur athlete as it would be for a professional.
The timer went off with a loud “Ting!” and Wildermuth carefully unwrapped Joe’s knee. The skin was bright pink from the ice. Motioning for Joe to sit at the end of the table, Wildermuth explained he was going to begin the therapy with an exercise designed to increase the range of motion in the knee and to strengthen the muscles above and below the joint. Putting his hands around Joe’s ankle, Wildermuth called out, “Kick up!” and as the therapist applied a weak resistance Joe slowly straightened out his leg in a kicking motion. “Kick down!” Wildermuth commanded, shifting his grip, and Joe forced his leg back down until it hung at a right angle once more. “Kick up!” Wildermuth commanded again, and Joe repeated the exercise. The shrunken muscles above his knee bulged with the effort, and by the time he had repeated the exercise fifteen times, they were aching.
After repeating the exercise a few more times, Wildermuth led Joe over to one of the clinic’s two Cybex machines, at $15,000 each the Cadillac of physical therapy equipment. The Cybex is basically a pair of red vinyl chairs with chrome-plated steel bars sticking up at odd angles around them. The patient sits in one of the chairs and manipulates the bars, which create resistance when they are moved up and down, rather like rowing with an oar or lifting weights. Through a complex hydraulic mechanism, the resistance of the bars can be adjusted high or low, and at any setting they also create more resistance the faster they are moved, so that a healthy patient will work against a higher resistance while a weak patient automatically encounters less. This ‘‘variable resistance” is one advantage the Cybex has over conventional therapy equipment, but there are others, too. For one thing, the bar’s resistance is steady all the way through the motion — there are no sudden jerks or pulls as there are in weightlifting, for instance — which allows a patient to exercise his injured limb faster, harder, and with less pain. For another, the various motions of the Cybex bars are designed specifically to strengthen certain muscle groups, the same groups that are most weakened by an injury. (The chairs on a Cybex are used for strengthening the ankle, knee, and hip; a separate ‘‘upper extremity table” covers the shoulder, elbow, and wrist.)
Joe sat down in one of the red vinyl chairs, and both he and I were surprised when Wildermuth first strapped Joe’s uninjured left leg to one of the Cybex bars. One strap went around his ankle and another around his thigh. “We have to measure your good leg first to find out what your normal strength is,” Wildermuth explained. “That’s another one of the great things about the Cybex; we can use it for both training and testing. It gives us the best objective test for strength a physical therapist ever had.”
There was a whir as Wildermuth turned on the Cybex, and then he told Joe to work the bar up and down fifteen times as fast as he could, using a kicking motion similar to the previous exercise. Joe’s efforts printed out on a nearby roll of paper like the jagged lines on a seismograph, only here the peaks and valleys indicated the maximum resistance created in foot-pounds of torque. Then Wildermuth connected Joe’s right leg to the bar and told him to work it up and down fifteen times. Wildermuth compared the results of this test with the previous one and announced that Joe’s right leg was only forty percent as strong as his left. Joe just shook his head, breathing hard.
After that, Wildermuth had Joe repeat the exercise with his right leg, and called out, “One! Two! Three!’’ as Joe kicked up and down as fast as he could. Wildermuth held his flattened palm out in front of the machine and the tips of Joe’s toes came up and just barely touched it at the top of each stroke. Joe had to grip the seat with both hands to gain leverage, and he squirmed and bounced in the chair with the effort. Afterward, as Joe sat puffing in the chair, Wildermuth smiled. “You know, when I played football in the ’50s, nobody even. knew what a weight room or a Cybex machine was,’’ he remarked. “People used to do jumping jacks to try to build up their muscles and stay in shape. There was no scientific background to it; they just did them because they had done them in high school. But you really need to understand physiology to be able to rehabilitate an injury.’’
Next Wildermuth had Joe work out on an exercycle for fifteen minutes, and by the end of that Joe was complaining that his knee hurt a little. Wildermuth fastened another ice-filled towel on it, and the day’s treatment had come to an end. Fifty-five minutes, thirty-five bucks (the clinic’s average cost for an hour of therapy).
“We accommodate about fifty to sixty separate treatments a day,” Wildermuth told me later, “and the average treatment takes about an hour. For a serious injury like a knee cartilage tear, our goal is to have the patient at about eighty percent strength after six to eight weeks. But it varies a lot depending on the individual, what kind of shape he was in when he was injured, how bad the injury was, and so forth.
“Would a clinic like this have been successful ten or fifteen years ago? Perhaps not — at least not on this scale. San Diego is a very active community for running, golf, racquetball, surfing. . . . And that interest in physical recreation definitely provides us with more patients.”
Over the next few weeks Wildermuth kept track of Joe’s progress by checking the resistance his leg generated on the Cybex, and also by measuring his leg muscles. Within a few weeks Joe found that his knee was strong enough to allow him to swim and even to play a little tennis. His visits to the Sports Injury Clinic decreased from three times a week to two, and finally to one. “Eventually,” Wildermuth says, “you get to the point where you no longer need this intensive care. You can get by with a less structured [and less expensive] rehabilitation program, and at that point we’ll recommend that a patient go to any one of several athletic clubs, like the Family Fitness Centers or Phil Tyne’s. . . .”
Phil Tyne is a boyish-looking man of thirty-three, with a catlike smile that seems to be perpetually on his face. As you might expect from someone in his profession, he believes strongly in the importance of exercise. Once, while he was in the Navy, Tyne convinced his commanding officer to convert the brig of an attack landing craft into a small gym. Later he obtained his B.A. at San Diego State while studying to be a trainer under Dr. Robert Moore, and subsequently worked for the Sports Injury Clinic and a chain of health clubs before going to work three years ago as the conditioning coach for the San Diego Chargers. At that time Tyne was pursuing his Master’s degree in athletic medicine at State, a pursuit he never finished. “Once I got hired by the Chargers,” he explains with a laugh. “I kind of lost my incentive.” Two and a half years ago he opened his own athletic club in the Cabrillo Building, at the comer of Ninth and Ash downtown.
Tyne’s club consists of two main exercise rooms, with separate locker rooms upstairs for men and women. The walls of the exercise rooms are adorned with pictures of Tyne standing with “Mean” Joe Green, Tyne standing with John Jefferson, Tyne standing with Russ Washington and Doug Wilkerson. et cetera. The rooms themselves are full of mats, benches, bars, weight racks, and four ornate exercise machines called CAM II. at $2000 each sort of an economy-model Cybex that runs off compressed air. Like the Cybex, the pressure on the CAM II exercise bars can be adjusted to create various amounts of resistance.
I met Tyne at his club one afternoon not long ago, and amid the clink of weights and the bantering of customers in the background he told me, “I get a lot of racquetball players in here who tell me their shoulders are hurting, their elbows are hurting. ... I ask them if they warm up before they play, and they say, ‘Oh yeah, we hit the ball around for ten minutes.’
He laughed. “The sport itself is not going to warm them up. And this is the problem with tennis players, too, and joggers. People don’t take the time to stretch out, warm up before they exercise. You've got to get circulation in the joints first, loosen up those muscles. There’s a direct correlation between tight muscles and knee damage, for instance.”
Since were were on the subject of knee damage, I asked Tyne how he went about rehabilitating and conditioning an injured amateur athlete like Joe. He replied that after getting a report from the Sports Injury Clinic on how well the individual had done or was doing in therapy, he himself would measure the injured area — in Joe’s case the muscles around the knee. After that he would test the strength of the injured limb on the CAM II equipment, and would then devise an exercise program with the number and difficulty of the exercises tailored to the individual's strength. To illustrate the wide difference in people's strengths, Tyne recalled that he was in the Chargers’ training room one day when Doug Wilkerson flexed a Cybex bar so fast and so hard it broke the machine’s metering device. On the other hand, he said, he’d recently had one young woman at his club who, after an operation to remove varicose veins, couldn’t even lift the free weight of the CAM II bar with her leg. With the machine turned off the bar weighs only a pound. “Eventually you increase the resistance [of the CAM II] but have the person do fewer repetitions,” Tyne continued. He emphasized again that different people work with different limits of resistance, but noted, that “for someone who’s been injured, the upper limit on resistance is pain. You don’t want to get any muscle soreness and you sure don’t want to get any pain, because pain is the body telling you that something's wrong.”
Once his customers have worked up sufficient strength in their injured limbs, Tyne has them begin exercises designed to prepare them for the particular sport they want to play. “You try to train as specific as you can.” he said. “It’s called the Laws of Specificity. A racquctball player wouldn't be doing the same thing as a football player or a runner. You try to simulate the motion and weight of the individual sport as closely as you can.” Since Joe primarily wants to resume his skiing. Tyne has set up an exercise program for him that includes “wall sitting” — squatting with your back pressed against a wall, a position that imitates a skier crouched on his skis. Tyne also lays down two wooden blocks on the floor, a foot apart, and has Joe hop sideways through them, both feet at a time, first one way and then the other. And Tyne has Joe working out on the Total Gym, too, a black vinyl-and-chrome bench tilted at a thirty-degree angle. The seat of the Total Gym slides up and down on rails, enabling you alternately to bend your legs and straighten them, lifting your body up and down on first one leg and then the other.
“You can’t prevent injuries, but you can increase the odds of not having them,” Tyne insisted. “The key is flexibility and strength. Any time you have an injury you lose muscle strength and size — and range of motion. So in rehabilitation you concentrate on getting those things back. How long do you have to continue exercising after an injury? Well, maybe the rest of your life, because as soon as your muscles get weak you could have a problem.”
The last time I saw Joe he was standing in one of the exercise rooms at Tyne’s athletic club, rubbing his face with a towel after a hard workout; his gray Syracuse University T-shirt was soaked through with sweat. I asked him if he felt he had come back from his injury one hundred percent, if all his therapy and conditioning had worked. “I really think so,” he nodded. “I went skiing just last weekend and didn't feel a thing. Not a twinge. It was great.”
But Joe added ruefully he’s been playing so much tennis lately to stay in shape that his elbow is getting sore. And he feels like he must have strained something in his lower back, too. He doesn’t really know what it is; it just hurts. “Phil says I just need more exercise,” he told me with a wry smile. “Arm curls, Williams’s Flexion routine — something like that.” He shrugged and turned toward the stairway to the locker room.
Joe, Joe, you’re getting older, Joe. Better take it easy on that body of yours. You can’t do all those things you could when you were younger.
Here's something you might be interested in.
What San Diegans do now when knee cartilage tears
The rise and falls of the amateur athlete
What San Diegans do now when knee cartilage tears
The rise and falls of the amateur athlete
Arthroscopic surgery engenders professional jealousy among some colleagues.
Flexibility and strength. Range of motion. These are the keys to avoiding any athletic injury, or so claims Phil Tyne. Tyne owns an athletic club in downtown San Diego and he is also the conditioning coach for the San Diego Chargers; you have to believe he knows something about athletic injuries.
“It’s weekend and amateur athletes who get hurt the most."
Professional athletes get injured often enough these days, he concedes, but they would get injured a lot more often if they weren’t in excellent physical condition. “Actually, pro athletes have an advantage; they can work at staying in shape seven days a week,” Tyne says. “It’s weekend and amateur athletes who get hurt the most. You leave your office on Friday evening and the next day you’re out running or playing racquetball or soccer. And in the heat of competition you maybe have to stretch further than you ever have in your life. You overdo it, and suddenly you're in a situation you can't get your body out of.’’
Phil Tyne: “You can’t prevent injuries, but you can increase the odds of not having them.”
Take Joe, for example, one of Tyne’s current customers at the club. Joe is thirty-five years old. six feet, two inches tall, and just a shade over 200 pounds. He has the dark hair and quick, sarcastic wit you often associate with people from the East Coast, and as a matter of fact that’s where he’s from — Syracuse, New York.
Removing bits of torn knee cartilage remains one of the commonest and most practical applications for the new surgical technique.
Joe (not his real name) used to play a little football in high school and college, but ever since he passed the bar exam and moved out to San Diego he hasn’t had much time to stay in shape.
Byron Wildermuth: “We go through a lot of ice here.”
You might have seen his law office in Hillcrest — one of those converted Victorian houses with beveled glass windows, carpets an inch thick, and a lot of expensive antique furniture.
Well, three months ago Joe went skiing for the first time in two years and got his body into a situation he couldn’t get it out of. Technically, of course, he did get out of it, but not before ripping apart the cartilage in his right knee. Now, after surgery, a short period of rest, and six or seven weeks of rehabilitation therapy, he’s trying to work himself into good physical condition at Tyne’s club.
“We’re not doctors and we’re not physical therapists,” Tyne tells potential customers like Joe who have had serious injuries. “We don’t cure anybody in here. But we’ll work as closely with your previous therapy as we can, and we’ll strengthen the affected area as much as possible. The better shape you’re in, the less likely it is you’ll re-injure yourself.” So Joe comes down to Tyne’s club once a week and strains and puffs along with overweight businessmen and housewives, fine-looking college athletes (both women and men), and a couple of people recuperating from injuries such as his own.
It costs him additional time and money on top of the three months and thousands of dollars he’s already spent on surgery and rehabilitation therapy, but if you bring up that subject, Joe will just laugh and say he’s only doing his part. The American public’s modern penchant for physical recreation has led to a burgeoning number of athletic injuries, and this in turn has led to increasing work for orthopedic surgeons, new surgical techniques, special therapy clinics with even more specialized equipment, and even experts like Tyne who concentrate just on trying to prevent injuries. Only ten or fifteen years ago Joe would have had an operation and afterward would have been more or less on his own. “Oh, the doctors might have told me to wait six weeks and then give my knee some exercise, but most of them wouldn’t have been able to say exactly what I should do,” Joe told me one evening after his workout at Tyne’s club. “The way I figure it, I was probably lucky to injure myself in 1981.”
The scissors that clipped Joe’s torn cartilage and removed it from inside his knee are the size and shape of a large screwdriver. By pressing a lever on the handle, tiny blades on the end of the long, needlelike point can be opened and closed almost effortlessly. I saw the scissors not long ago in the office of Dr. Rory Bergen, one of several orthopedic surgeons in San Diego with extensive experience in athletic injuries. Bergen pulled the instrument from a box that was stored behind his desk and said with a mischievous smile, “To stay current in this business you really have to be something of a gadgeteer.” Then he deftly snipped two small V-shaped notches in an invoice on his desk to show me how sharp the scissors are.
“There are a lot more people coming in to see orthopedic surgeons these days,” Bergen told me. “Athletic injuries are on the increase because of the population increase in general, and also because of the fitness renaissance. But one of the biggest reasons has been the increasing involvement of women in athletics. In a way, they have sort of doubled the population,” or at least doubled the number of patients for orthopedic surgeons.
Most of the patients Bergen sees have serious injuries — torn ligaments or cartilage, or badly broken bones. To correct these problems he employs arthroscopic surgery, a new technique which seems to have clear-cut advantages over the old operating methods. But it is a technique which also engenders professional jealousy among some colleagues, and so Bergen requested that his true name not be used in this article (it isn’t). Some doctors who still use the old techniques feel threatened by the new ones, he said, and part of the reason could be the considerable investment of time (for learning) and cash (about $15,000 worth of equipment) that arthroscopic surgery requires. If Bergen’s true name were to appear here, some doctors might accuse him of being on an ego trip or advertising “his” methods through the media. “And in a way they’d be right, because a lot of people read your paper, and it would amount to an inadvertent advertisement,” Bergen told me. “And frankly, I don’t want that at all. I’m always behind schedule; I’ve got more patients than I want already. But on the other hand, I think all doctors will be using these techniques in five years, and I think the public has a right to know about them.”
Arthroscopic surgery employs the kind of specialized, sophisticated instruments that laypersons are amazed to learn even exist. These instruments have enabled surgeons to reconstruct torn ankle, knee, and shoulder ligaments from a patient’s tendons, and also, in some cases, to sew ligaments together. Bergen says that someday soon surgeons using arthroscopic surgery might even be able to sew torn cartilage back together. For the time being, however, removing bits of torn knee cartilage remains one of the commonest and most practical applications for the new surgical technique.
The cartilage in your knee is a rubbery tissue that lubricates and cushions the area where the femur (upper leg) rests upon the tibia (lower leg). According to Bergen, the cartilage distributes the weight of the upper body in a remarkably efficient way. “Studies have shown that the pressure goes up fantastically high without any cartilage in there,” he says. But because most cartilage has no blood vessels in it, and thus doesn’t receive nutrients, it cannot heal when damaged; and torn cartilage, if left in the knee, can cause the joint to buckle, lock up, and otherwise malfunction.
Until recently, Bergen explains, if X rays disclosed that you had torn your knee cartilage, you would have gone to a hospital and had the entire cartilage removed through a two-inch incision in your knee. “But a number of us became increasingly dissatisfied with that, because long-term studies showed that with full removal of the cartilage, fifteen or twenty years down the line a high percentage of patients would complain of pain and restricted motion in their injured knees. But on the other hand, it’s difficult to remove only a part of the cartilage with a skin-incision-type operation.”
According to Bergen, it wasn’t until 1974 that an instrument was perfected which enabled surgeons to look directly inside of knees and other joints without cutting them open. Called an arthroscope, it looks a little like a periscope with the eyepiece attached to the upper part. The bottom part is a pointed rod with a light and a magnifying lens at the end, and it can be inserted directly into a joint. The surgeon peers through the eyepiece and can examine the injured area virtually at his leisure. (“Unlike some joints, the knee has a lot of space inside it,” Bergen told me when I asked. “It’s like a little room in there.”)
About the same time the arthroscope was invented, microsurgical instruments were developed which allowed surgeons to perform much finer and more delicate operations than before. Orthopedic surgeons soon became interested in utilizing these instruments in combination with the arthroscope for a variety of operations, and arthroscopic surgery was born. Bergen says that much of the modem surgical technique for removing only part of a knee cartilage was pioneered by Dr. Richard O’Connor of Inglewood, California, and adds with a note of awe in his voice that O’Connor died of cancer recently “after having done at least 2900 knees.”
When Joe first showed up at Bergen’s office, he complained that his knee had been giving him problems ever since he had taken a spill while skiing a few weeks earlier. It didn’t really hurt that much, he said, it just didn’t seem to be working right. Bergen asked him to describe the accident, and the full story, as Joe described it to me later, went like this:
Right after Christmas last year he and his wife Sherry drove up to Mammoth for three days of skiing. It had been a dry winter so far, and they could see rocks here and there sticking up out of a shallow, twenty-inch base of snow. After the first morning, Sherry decided to catch up on her reading at the condominium they’d rented, but that afternoon Joe took the lift up to the Cornice. He’d never been up to the Cornice, a dangerously steep slope for experienced skiers, but it was the highest slope at Mammoth, and Joe reasoned that the higher he went the more snow he’d find. He was right, but there were still a few rocks dotting the snow as he pushed off down the run. The first part of the Cornice is a nearly vertical drop, and for thirty feet or more Joe’s skis never even touched ground. After that he was rocketing down the slope, faster than he’d ever gone before, the wind stinging his nose and cheeks like a caustic chemical. He turned quickly left, then right, and was leaning into the hill to turn left again when his skis hit a rock and he started to slide. Instead of falling, he straightened up and tried to regain his balance, a trick he’d employed with much success on smaller slopes. This time, though, the edge of his right ski dug into the snow, the binding didn’t release, and for one awful instant Joe’s leg was anchored to the hill while the rest of his body twisted up into the air. He felt a hot, searing pain in his knee, and then he was airborne. “All I could see was my skis and blue sky. I knew I was going to hit ground soon and that I better do something about it. But, oh mother, the pain in my knee. . . .”
By the time Joe had skidded to a halt, the pain had virtually subsided. He even got up and finished the run. His knee felt weak, but not as if he had seriously damaged anything. Still, he was a little shaken up, and he called it a day and made his way back to Sherry and the condo.
The next morning his knee was swollen the size of a cantaloupe. Sherry was appalled, and all the way back to San Diego she kept telling Joe he must have done something really bad to it, that he’d better go see a doctor right away. But Joe’s the kind of guy who’s always had, well, not exactly a fear of doctors, but a strong dislike. He’d hurt himself a few times playing football, but he’d never gone to a doctor then and things had always turned out fine. So he held off, and for a few weeks his knee actually seemed to be getting better. The swelling went away, and even though he couldn’t put much weight on it he could get around with the help of a cane. But one afternoon he was getting out of a car in front of his office and his knee just seemed to freeze up. No matter what he did he couldn’t get it to straighten out, and finally he decided he’d pay a visit to someone like Bergen.
Bergen could see that Joe’s right leg was already beginning to grow thin from lack of use. When the X rays showed no broken bones, bone chips, or anything else in the knee, he asked a few more questions and ran a few more tests, and then told Joe that it looked like a torn cartilage. Bergen said he would schedule an arthroscopy for the following week and could remove the torn part of the cartilage then. Joe just nodded and went home to bite his nails.
The operation to remove Joe’s torn cartilage went as smoothly as it could. Joe showed up at the hospital at nine in the morning and was out cold by ten. Bergen shaved the injured right knee with a little lawnmower-like device that cuts hair and sucks it up through a vacuum hose, and then used a syringe to inject Joe’s knee with saline solution. Soon the joint was swollen to twice its normal size — a painful but necessary step that gives the surgeon more room to work and is the main reason for keeping the patient unconscious throughout the operation. After that Bergen put in the arthroscope.
“This surgery is designed to preserve as much of the cartilage as possible,” Bergen explains. “Technically, it’s super-difficult for the surgeon. It’s tedious. It takes a long time to learn, and you have to be patient.” Peering through the arthroscope, the surgeon searches the inside of the knee for the torn piece of cartilage. Once he locates it he punches two more holes in the skin of the patient’s knee, one for the blunt-nosed “hook” and one for scissors. Staring through the arthroscope the entire time, he maneuvers the hook under the torn cartilage and lifts it up. “Then,” says Bergen, “you reach the scissors in through the other hole, snip off the torn part, and extract that baby right through the skin.” On the average, the operation takes Bergen about forty minutes, and at least once he has affixed a video camera to the arthroscope and maneuvered his instruments while watching them on closed-circuit TV. “Aside from joint implants, it’s one of the most exciting things that’s happened in orthopedics recently,” he says with genuine eagerness.
Including the use of the hospital facility for half a day, the anesthesiologist’s fee, and the surgeon’s fee, the operation costs in the neighborhood of $2000. But Bergen figures that’s still cheaper than the old operation, which requires a hospital stay of two or three days as well as a surgeon’s fee and other costs. In addition, a patient who has had his entire cartilage removed is usually on crutches for one week and is unable to exert himself physically for four to six weeks. But the patient who undergoes a partial cartilage removal, Bergen claims, “winds up with three stab wounds instead of an incision. Usually he can walk away from the operation once the anesthetic wears off. He can go to work the next day.
“The disadvantage is that you might leave cartilage behind that could tear again, but that doesn’t seem to be happening,” he continues. “We don’t really know what the long-term results will be, because the techniques just haven’t been around that long. But to me there’s no question that the results will be comparable to or better than the old operation.”
A week after his operation Joe was back in Bergen’s office for a checkup, thanking him and saying that his knee felt a lot better. But because Joe had waited so long to have it operated on, Bergen advised him to see a physical therapist to build up his atrophied leg muscles. He recommended a place called the Sports Injury Clinic, which specializes in rehabilitating athletic injuries. “The most important thing for you to do after a knee injury,” Bergen emphasized as Joe was leaving his office that evening, “is to get your muscles rehabilitated.”
Joe recalls that when Bergen first mentioned the Sports Injury Clinic, his first thought was: “You’re kidding — a clinic just for sports injuries?” He concluded it must be a place where local college and professional athletes go to recuperate from their battle wounds, and he joked with Sherry about sitting on an exercycle next to Louie Kelcher or Ozzie Smith, bantering about bygone Super Bowls or World Series. It didn’t turn out that way.
The Sports Injury Clinic is housed in a new shopping center complex on Aero Drive, just south of Montgomery Field. There is a Japanese restaurant on one side and a film processing shop on the other. You enter through double glass doors and find yourself in a wide, open room furnished in a way that might be described as “pleasantly modern.” Everything that isn’t glass or natural wood seems to be gleaming chrome or vinyl. The walls are sparkling white and the rug is an earthy brown.
The clinic was founded three and a half years ago by Dr. Robert Moore, a teacher and trainer at San Diego State University, and Ric McDonald and Dick Dent, the Chargers’ and Padres’ trainers, respectively. Its current director, however, is Byron Wildermuth, a tall, confident man of forty-six with clear blue eyes and longish white hair that lends an air of distinction to his overall appearance. In addition to being the clinic’s director, Wildermuth (his real name) is a registered physical therapist, and personally supervises the rehabilitation programs for some of the clinic’s patients. “A clinic like this might seem like a new phenomenon, but it really isn’t,” he says. “Pro athletic teams have always had their high-priced doctors, trainers, and exercise equipment. We bring that expertise to the athlete who didn’t have access to this kind of thing before.” A few of the clinic’s patients are professional golfers and tennis players who don’t have access to team trainers, and in the past a few superstar athletes like Bill Walton and Willie Stargell have also used the facility. “But most of the patients here,” Wildermuth says, “are amateur and recreational athletes — the office-worker-runner-skier type. Most of them have some sort of mechanical problem with a joint — knees are the most common, then shoulders and ankles — but we treat sprains, tendonitis, everything down to tennis elbow.”
In addition to Dent, McDonald, and Moore, who work at the clinic part-time, the staff at the Sports Injury Clinic consists of Wildermuth and several certified athletic trainers. Athletic trainers need to pass a standard test to be certified at their profession, and some begin to prepare for that test as undergraduates at San Diego State, where a growing athletic medicine program includes classes in human physiology, corrective and orthopedic physical education, and weight training, among others. In order to gain a trainer’s certificate the students must also serve two years as an intern to a certified athletic trainer, a requirement most do not fulfill until after they’ve obtained their Bachelor’s degree. A physical therapist like Wildermuth needs to pass a certification test, too, and as an undergraduate takes classes similar to those taken by aspiring trainers. But his education includes less on-the-field experience in such specialties as first aid and taping, and his required internship with a registered physical therapist is only five months.
I accompanied Joe the first afternoon he went to the Sports Injury Clinic. After filling out the prescribed forms and handing over a “surgical report” prepared by Bergen, he chatted with Wildermuth about what type of surgery he had had, and whether or not he was still having any pain in his knee. Then Wildermuth directed him to the men’s dressing room. Joe returned a few minutes later wearing only athletic shorts and a T-shirt, and Wildermuth measured both of his knees, just above the kneecap. Joe seemed genuinely upset when he learned how much his injured leg had atrophied since his skiing accident; it was nearly two inches thinner than his good one. In fact it was a pasty, scrawny-looking thing, more like a child's arm than the leg of a grown man. The three small scars from his operation glistened on his knee like some sort of giant cobra bite.
Wildermuth next led Joe over to a row of vinyl-covered tables, a few of which were already occupied by other patients. Some of the patients were women dressed in dark-colored dancing tights with running shorts pulled on over them, and others were men dressed in shorts and T-shirts like Joe. Wildermuth indicated one of the empty tables, and Joe hoisted himself up on it and gingerly stretched out his right leg. Then Wildermuth brought over a towel filled with ice and proceeded to wrap Joe’s knee with it, fastening it in place with an elastic bandage. “We go through a lot of ice here,” Wildermuth explained as he worked. “About 1000 pounds a day. It’s called cryotherapy, and it’s really just an adjunct to our regular therapy. Ice increases the circulation and lessens fatigue.
It controls swelling, decreases spasms, and has a slight numbing effect that allows us to work you relatively pain-free.” When Joe asked if there were any injuries that heat was good for — as in Jacuzzis or hot whirlpools, for instance — Wildermuth shrugged. “I suppose so,” he said. “But we feel ice is better. You always put ice on an injury for the first forty-eight hours. Some people say you should apply heat after that, but we get better results with ice.”
When he had finished wrapping Joe’s knee, Wildermuth set a small plastic timer for fifteen minutes and then sat down in a chair next to the table. As the timer ticked away he told Joe that the other patients at the clinic had come in on their doctors’ recommendations. “We work on doctors’ referrals only,” he explained. “It’s like a prescription for drugs — your doctor gives us a diagnosis and a broad prescription for rehabilitation, and we take care of the specifics.” Treatment can vary from one day to eight weeks, he added, depending on the injury, and is virtually the same for an amateur athlete as it would be for a professional.
The timer went off with a loud “Ting!” and Wildermuth carefully unwrapped Joe’s knee. The skin was bright pink from the ice. Motioning for Joe to sit at the end of the table, Wildermuth explained he was going to begin the therapy with an exercise designed to increase the range of motion in the knee and to strengthen the muscles above and below the joint. Putting his hands around Joe’s ankle, Wildermuth called out, “Kick up!” and as the therapist applied a weak resistance Joe slowly straightened out his leg in a kicking motion. “Kick down!” Wildermuth commanded, shifting his grip, and Joe forced his leg back down until it hung at a right angle once more. “Kick up!” Wildermuth commanded again, and Joe repeated the exercise. The shrunken muscles above his knee bulged with the effort, and by the time he had repeated the exercise fifteen times, they were aching.
After repeating the exercise a few more times, Wildermuth led Joe over to one of the clinic’s two Cybex machines, at $15,000 each the Cadillac of physical therapy equipment. The Cybex is basically a pair of red vinyl chairs with chrome-plated steel bars sticking up at odd angles around them. The patient sits in one of the chairs and manipulates the bars, which create resistance when they are moved up and down, rather like rowing with an oar or lifting weights. Through a complex hydraulic mechanism, the resistance of the bars can be adjusted high or low, and at any setting they also create more resistance the faster they are moved, so that a healthy patient will work against a higher resistance while a weak patient automatically encounters less. This ‘‘variable resistance” is one advantage the Cybex has over conventional therapy equipment, but there are others, too. For one thing, the bar’s resistance is steady all the way through the motion — there are no sudden jerks or pulls as there are in weightlifting, for instance — which allows a patient to exercise his injured limb faster, harder, and with less pain. For another, the various motions of the Cybex bars are designed specifically to strengthen certain muscle groups, the same groups that are most weakened by an injury. (The chairs on a Cybex are used for strengthening the ankle, knee, and hip; a separate ‘‘upper extremity table” covers the shoulder, elbow, and wrist.)
Joe sat down in one of the red vinyl chairs, and both he and I were surprised when Wildermuth first strapped Joe’s uninjured left leg to one of the Cybex bars. One strap went around his ankle and another around his thigh. “We have to measure your good leg first to find out what your normal strength is,” Wildermuth explained. “That’s another one of the great things about the Cybex; we can use it for both training and testing. It gives us the best objective test for strength a physical therapist ever had.”
There was a whir as Wildermuth turned on the Cybex, and then he told Joe to work the bar up and down fifteen times as fast as he could, using a kicking motion similar to the previous exercise. Joe’s efforts printed out on a nearby roll of paper like the jagged lines on a seismograph, only here the peaks and valleys indicated the maximum resistance created in foot-pounds of torque. Then Wildermuth connected Joe’s right leg to the bar and told him to work it up and down fifteen times. Wildermuth compared the results of this test with the previous one and announced that Joe’s right leg was only forty percent as strong as his left. Joe just shook his head, breathing hard.
After that, Wildermuth had Joe repeat the exercise with his right leg, and called out, “One! Two! Three!’’ as Joe kicked up and down as fast as he could. Wildermuth held his flattened palm out in front of the machine and the tips of Joe’s toes came up and just barely touched it at the top of each stroke. Joe had to grip the seat with both hands to gain leverage, and he squirmed and bounced in the chair with the effort. Afterward, as Joe sat puffing in the chair, Wildermuth smiled. “You know, when I played football in the ’50s, nobody even. knew what a weight room or a Cybex machine was,’’ he remarked. “People used to do jumping jacks to try to build up their muscles and stay in shape. There was no scientific background to it; they just did them because they had done them in high school. But you really need to understand physiology to be able to rehabilitate an injury.’’
Next Wildermuth had Joe work out on an exercycle for fifteen minutes, and by the end of that Joe was complaining that his knee hurt a little. Wildermuth fastened another ice-filled towel on it, and the day’s treatment had come to an end. Fifty-five minutes, thirty-five bucks (the clinic’s average cost for an hour of therapy).
“We accommodate about fifty to sixty separate treatments a day,” Wildermuth told me later, “and the average treatment takes about an hour. For a serious injury like a knee cartilage tear, our goal is to have the patient at about eighty percent strength after six to eight weeks. But it varies a lot depending on the individual, what kind of shape he was in when he was injured, how bad the injury was, and so forth.
“Would a clinic like this have been successful ten or fifteen years ago? Perhaps not — at least not on this scale. San Diego is a very active community for running, golf, racquetball, surfing. . . . And that interest in physical recreation definitely provides us with more patients.”
Over the next few weeks Wildermuth kept track of Joe’s progress by checking the resistance his leg generated on the Cybex, and also by measuring his leg muscles. Within a few weeks Joe found that his knee was strong enough to allow him to swim and even to play a little tennis. His visits to the Sports Injury Clinic decreased from three times a week to two, and finally to one. “Eventually,” Wildermuth says, “you get to the point where you no longer need this intensive care. You can get by with a less structured [and less expensive] rehabilitation program, and at that point we’ll recommend that a patient go to any one of several athletic clubs, like the Family Fitness Centers or Phil Tyne’s. . . .”
Phil Tyne is a boyish-looking man of thirty-three, with a catlike smile that seems to be perpetually on his face. As you might expect from someone in his profession, he believes strongly in the importance of exercise. Once, while he was in the Navy, Tyne convinced his commanding officer to convert the brig of an attack landing craft into a small gym. Later he obtained his B.A. at San Diego State while studying to be a trainer under Dr. Robert Moore, and subsequently worked for the Sports Injury Clinic and a chain of health clubs before going to work three years ago as the conditioning coach for the San Diego Chargers. At that time Tyne was pursuing his Master’s degree in athletic medicine at State, a pursuit he never finished. “Once I got hired by the Chargers,” he explains with a laugh. “I kind of lost my incentive.” Two and a half years ago he opened his own athletic club in the Cabrillo Building, at the comer of Ninth and Ash downtown.
Tyne’s club consists of two main exercise rooms, with separate locker rooms upstairs for men and women. The walls of the exercise rooms are adorned with pictures of Tyne standing with “Mean” Joe Green, Tyne standing with John Jefferson, Tyne standing with Russ Washington and Doug Wilkerson. et cetera. The rooms themselves are full of mats, benches, bars, weight racks, and four ornate exercise machines called CAM II. at $2000 each sort of an economy-model Cybex that runs off compressed air. Like the Cybex, the pressure on the CAM II exercise bars can be adjusted to create various amounts of resistance.
I met Tyne at his club one afternoon not long ago, and amid the clink of weights and the bantering of customers in the background he told me, “I get a lot of racquetball players in here who tell me their shoulders are hurting, their elbows are hurting. ... I ask them if they warm up before they play, and they say, ‘Oh yeah, we hit the ball around for ten minutes.’
He laughed. “The sport itself is not going to warm them up. And this is the problem with tennis players, too, and joggers. People don’t take the time to stretch out, warm up before they exercise. You've got to get circulation in the joints first, loosen up those muscles. There’s a direct correlation between tight muscles and knee damage, for instance.”
Since were were on the subject of knee damage, I asked Tyne how he went about rehabilitating and conditioning an injured amateur athlete like Joe. He replied that after getting a report from the Sports Injury Clinic on how well the individual had done or was doing in therapy, he himself would measure the injured area — in Joe’s case the muscles around the knee. After that he would test the strength of the injured limb on the CAM II equipment, and would then devise an exercise program with the number and difficulty of the exercises tailored to the individual's strength. To illustrate the wide difference in people's strengths, Tyne recalled that he was in the Chargers’ training room one day when Doug Wilkerson flexed a Cybex bar so fast and so hard it broke the machine’s metering device. On the other hand, he said, he’d recently had one young woman at his club who, after an operation to remove varicose veins, couldn’t even lift the free weight of the CAM II bar with her leg. With the machine turned off the bar weighs only a pound. “Eventually you increase the resistance [of the CAM II] but have the person do fewer repetitions,” Tyne continued. He emphasized again that different people work with different limits of resistance, but noted, that “for someone who’s been injured, the upper limit on resistance is pain. You don’t want to get any muscle soreness and you sure don’t want to get any pain, because pain is the body telling you that something's wrong.”
Once his customers have worked up sufficient strength in their injured limbs, Tyne has them begin exercises designed to prepare them for the particular sport they want to play. “You try to train as specific as you can.” he said. “It’s called the Laws of Specificity. A racquctball player wouldn't be doing the same thing as a football player or a runner. You try to simulate the motion and weight of the individual sport as closely as you can.” Since Joe primarily wants to resume his skiing. Tyne has set up an exercise program for him that includes “wall sitting” — squatting with your back pressed against a wall, a position that imitates a skier crouched on his skis. Tyne also lays down two wooden blocks on the floor, a foot apart, and has Joe hop sideways through them, both feet at a time, first one way and then the other. And Tyne has Joe working out on the Total Gym, too, a black vinyl-and-chrome bench tilted at a thirty-degree angle. The seat of the Total Gym slides up and down on rails, enabling you alternately to bend your legs and straighten them, lifting your body up and down on first one leg and then the other.
“You can’t prevent injuries, but you can increase the odds of not having them,” Tyne insisted. “The key is flexibility and strength. Any time you have an injury you lose muscle strength and size — and range of motion. So in rehabilitation you concentrate on getting those things back. How long do you have to continue exercising after an injury? Well, maybe the rest of your life, because as soon as your muscles get weak you could have a problem.”
The last time I saw Joe he was standing in one of the exercise rooms at Tyne’s athletic club, rubbing his face with a towel after a hard workout; his gray Syracuse University T-shirt was soaked through with sweat. I asked him if he felt he had come back from his injury one hundred percent, if all his therapy and conditioning had worked. “I really think so,” he nodded. “I went skiing just last weekend and didn't feel a thing. Not a twinge. It was great.”
But Joe added ruefully he’s been playing so much tennis lately to stay in shape that his elbow is getting sore. And he feels like he must have strained something in his lower back, too. He doesn’t really know what it is; it just hurts. “Phil says I just need more exercise,” he told me with a wry smile. “Arm curls, Williams’s Flexion routine — something like that.” He shrugged and turned toward the stairway to the locker room.
Joe, Joe, you’re getting older, Joe. Better take it easy on that body of yours. You can’t do all those things you could when you were younger.
Comments